 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
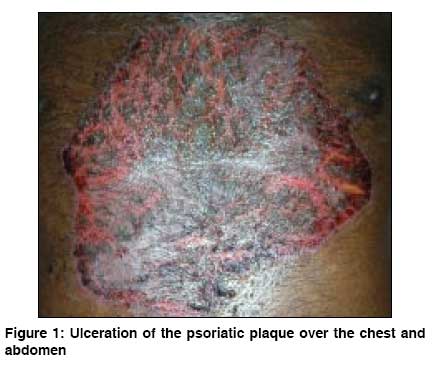
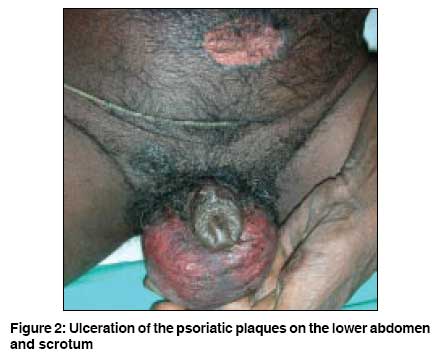
Indian Journal of Dermatology, Venereology and Leprology, Vol. 74, No. 5, September-October, 2008, pp. 481-484 Case Report Methotrexate toxicity presenting as ulceration of psoriatic plaques: A report of two cases Agarwal KishanKumar, Nath AmiyaKumar, Thappa DevinderMohan Department of Dermatology and STD, Jawaharlal Institute of Postgraduate Medical Education and Research (JIPMER), Pondicherry Code Number: dv08205 Abstract We describe two cases of methotrexate toxicity occurring due to inappropriate self-medication with the drug. The first patient was a 57-year-old man with plaque-type psoriasis on intermittent methotrexate therapy. He discontinued his medications for 2 months and had exacerbation of psoriasis for which he self-medicated with methotrexate following which he developed ulceration of the psoriatic plaques accompanied by bone marrow suppression. The second patient was a 68-year-old man with chronic plaque-type psoriasis for 20 years and was being treated with intermittent methotrexate for 15 years. He also self medicated with oral methotrexate 15 mg daily for 7 days for exacerbation of psoriasis and developed ulceration of the psoriatic plaques with bone marrow suppression and evidence of gastrointestinal erosions.Keywords: Methotrexate toxicity, Psoriasis, Skin ulceration Introduction Methotrexate is a potentially toxic antimetabolite anticancer drug, [1] which, in low doses, remains an effective and safe therapy for psoriasis, if careful monitoring is done according to the recommended guidelines. [2] Failure to adhere to the guidelines can lead to methotrexate toxicity. Well-known signs of methotrexate toxicity include bone marrow suppression and oral and gastrointestinal ulcerations. [3] Ulceration of psoriatic plaques is a less common sign of methotrexate toxicity. [3] Herein we describe two cases of methotrexate toxicity presenting with bone marrow suppression and ulceration of psoriatic plaques.Case Reports Case 1 On physical examination, the patient was febrile (102° F), but conscious. Skin examination revealed ulceration of the psoriatic plaques over scalp, chest, abdomen, and upper and lower limbs (approximately 25% of his body surface area) [Figure - 1]. There was no evidence of mucositis or any hepatosplenomegaly. His pulse rate was 110/minute and respiratory rate was 40/minute, otherwise his systemic examination was unremarkable. Laboratory studies revealed a hemoglobin of 10.9 g/dL, red blood cell count of 4.15 lacs/µL, mean corpuscular volume of 96 fL, white blood cell count (WBC) of 600/µL and the platelet count of 16,000/µL. Serum biochemistry showed a serum creatinine level of 0.8 mg/dL, blood urea nitrogen of 35.0 mg/dL, and total bilirubin of 2.4 mg/dL with direct bilirubin of 1.2 mg/dL, SGOT of 237 IU/L, SGPT of 205 IU/L, and alkaline phosphatase of 113 IU/L. Prothrombin time and partial thromboplastin time were within normal limits. Urine and stool analysis, chest x-ray and electrocardiogram were normal. Blood culture grew Staphylococcus aureus , which was sensitive to only vancomycin. Based on the above clinical and laboratory findings, a diagnosis of methotrexate toxicity was made. The patient was started on intravenous leucovorin calcium, 25 mg every 6 hours on day 1, followed by 10 mg every 6 hours on day 2 and 3. He was given filgrastim (G-CSF) at a dose of 5µg/kg/day administered subcutaneously until absolute neutrophil count reached 10,000/µL. He was also supported by transfusions of platelets and systemic antibiotics and antifungal therapy. Skin care consisted of daily cleaning with povidone iodine followed by application of silver sulfadiazine cream. Fever subsided 4 days after admission and repeat blood culture was sterile. The platelet count increased to 1,74,000/µL and WBC count increased to 34,600/µL within 7 days after admission. The ulcerated skin lesions began to heal within 4 days and complete healing occurred after 14 days. Six weeks later, the patient was started on methotrexate at 7.5 mg/week without any complications. Case 2 A 68-year-old man with a 20-year history of chronic plaque-type psoriasis had been treated with methotrexate (cumulative dose being 1850 mg) intermittently for 15 years. He discontinued his medications for 6 months and had exacerbation of psoriasis with appearance of multiple new lesions for which he self medicated with oral methotrexate 15 mg daily for 7 days. On the 5 th day, the patient developed ulceration of the psoriatic plaques on chest, abdomen, axilla, both elbows and scrotum. He also had painful pus filled lesions over palms and soles, and colicky abdomen with black tarry stools. On examination, the patient was conscious and normotensive. His pulse rate was 90/minute, temperature was 99°F, and respiratory rate was 40/minute. Cutaneous examination revealed approximately 10% of his skin surface was involved by ulcerated psoriatic plaques over the scalp, chest, abdomen, bilateral upper and lower limbs, sacral area, axilla and scrotum [Figure - 2]. Palms and soles had tender pustules. He had mild epigastric tenderness. His other systemic examination was unremarkable. Laboratory studies revealed a red blood cell count of 3.85/µL, hemoglobin of 9.6 g/dL, white blood cell count was 400/µL and the platelet count was 8,000/µL. A chemistry screen showed: serum creatinine - 0.8 mg/dL, blood urea nitrogen - 35.0 mg/dL, total bilirubin - 2.0 mg/dL, direct bilirubin - 1.2 mg/dl, SGOT - 210 IU/L, SGPT - 242 IU/L, and alkaline phosphatase 173 U/L. Prothrombin time and partial thromboplastin time were within normal limits. Stool was positive for occult blood. Urine analysis, chest x-ray and electrocardiogram were normal. Blood culture was sterile. On the basis of the above clinical and laboratory parameters, a diagnosis of methotrexate toxicity was made. The patient was started on filgrastim at 5µg/kg/day subcutaneously, intravenous ceftazidime 1 gm 8 th hourly, and oral fluconazole 150 mg daily. He was also supported by transfusions of platelets. Topical skin care consisted of daily cleaning with povidone iodine followed by application of silver sulfadiazine cream. The patient left the hospital against medical advice after 3 days. At that time, his clinical status was almost as it was at the time of admission. Discussion Methotrexate is an effective but potentially toxic treatment for psoriasis. [3] It has been in use since 1960s and dermatologists have generated an impressive record of safety with careful monitoring. [4] Low dose methotrexate therapy used in psoriasis rarely produces toxicity, and most of such cases occur due to failure to adhere to the recommended guidelines. [2] Myelosuppression and gastrointestinal mucositis are primary toxic effects of methotrexate. [1] The mucosal cells are more sensitive to methotrexate than the precursor cells in the bone marrow because of greater accumulation and persistence of methotrexate in the intestinal epithelium. Mucositis usually appears 3-7 days after the drug administration and precedes the onset of fall of leucocyte and platelet counts by several days. [1] Ulceration of the psoriatic plaques in the skin due to methotrexate toxicity is extremely rare. In a review of the literature from 1951 to 1996, Pearce and Wilson [3] found 64 patients, including two of their own patients, who had experienced cutaneous erosions believed to be secondary to methotrexate toxicity. Initially the psoriatic plaques become painful and red, and then develop superficial erosions. [3] These changes may be misdiagnosed as a flare of psoriasis [3] or an acute episode of pustular psoriasis, [5] both of which can lead to an increment of methotrexate dosage. Patients with psoriatic ulceration usually have more pain than expected from the superficial appearance of the lesions. [3] Ulcerations are restricted to the psoriatic plaques probably because of higher uptake of methotrexate by the hyperproliferative psoriatic plaques than normal skin. [6] However, many cases reported in the literature had some other form of cutaneous pathology existing before ulceration, either as a result of previous physical insults or as an underlying dermatosis. [7] Lawrence and Dahl [5] described 2 patterns of skin ulceration in patients with psoriasis being treated with weekly methotrexate: type I ulcers wherein the psoriatic plaques eroded shortly after starting methotrexate; and type II ulcers of the skin clinically not involved by psoriasis but affected by some other pathology such as scars. In both types, the pathogenic mechanism was thought to be direct toxicity of the drug. Skin ulcerations within the psoriasis plaques usually occur within one month of starting or restarting therapy, [5] however, such events have been reported following chronic administration of methotrexate. [6],[8] Healing is rapid with complete re-epithelialization occurring within 10-12 days after discontinuation of methotrexate. [5] Treatment of choice for bone marrow suppression secondary to methotrexate toxicity is leucovorin calcium, [2],[3] which is administered orally or intravenously every 6 hours after an immediate loading dose of 20 mg (10 mg/m 2 ) until plasma methotrexate concentration is 5x10 -8 or less. [1],[2] However, leucovorin calcium must be administered within 12-24 hours after the last dose of methotrexate to be effective. [3] Several factors have been identified which can precipitate methotrexate toxicity. The most common risk factors are an alteration in methotrexate dosage and the use of non-steroidal anti-inflammatory drugs. [3] Other possible contributing factors are renal insufficiency (because methotrexate is excreted unchanged primarily by the kidneys), infection, pustular flare of psoriasis and older age (55 years or more). [3] Drugs can increase the risk of methotrexate toxicity either by decreasing renal elimination of methotrexate (aminoglycosides, cyclosporine, non-steroidal anti-inflammatory agents, sulfonamides, probenecid, salicylates, penicillins, colchicines, cisplatin and other renotoxic drugs), or by displacing methotrexate from protein binding sites in the plasma (salicylates, probenecid, sulfonamides, barbiturates, phenytoin, retinoids, sulfonylureas, tetracyclines). [4] Synergistic toxicity can occur when methotrexate is used with trimethoprim-sulfamethoxazole, ethanol and pyrimethamine. [4] Daly et al , [9] and Groenendal and Rampen [10] reported cases of methotrexate toxicity which occurred due to co-administration of azapropazone and trimethoprim-sulfamethoxazole, respectively. Ng et al . [11] described a patient who developed necrotic skin ulceration and pancytopenia after concurrent administration of methotrexate, trimethoprim, and naproxen. The risk of toxicity secondary to methotrexate is even greater if additional methotrexate is administered sooner than the usual scheduled weekly dose, because a new population of dividing cells in the S phase will be targeted. [12] Rapidly proliferating cells have a greater susceptibility to methotrexate because more cells are in the S phase, where methotrexate exerts its effect. [13] Cell turnover is increased in psoriasis, but this rate is even higher when psoriasis is flaring. This may explain why the majority of cases of erosive psoriasis occurred when methotrexate therapy was interrupted which possibly led to a flare in their psoriasis, with more rapid cell turnover and more epidermal cells in the S phase. Campalani et al . [14] opined that specific common polymorphisms in folate, pyrimidine, and purine metabolic enzymes are associated with methotrexate efficacy and/or toxicity in psoriasis patients. Infection may be a risk factor for bone marrow toxicity because the bone marrow is producing more neutrophils, thereby increasing the number of susceptible cells. [15] Our patients were similar in many ways to those previously discussed. Both patients used methotrexate irregularly, were of older age, and had exacerbation of psoriasis because of which methotrexate dosage was increased. Methotrexate toxicity in our cases was an iatrogenic adverse event due to medication error. [16] Undoubtedly, methotrexate is associated with significant preventable medication errors that warrant careful measures to improve patient safety. While some of the errors could happen for any drug and be hazardous, the distinctive weekly or cyclical dosage scheme and low therapeutic index constitute the most clearly identifiable risks of methotrexate and accounts for the largest number of preventable serious injuries and deaths. [16] Dispensing methotrexate in the weekly dosage pack and communicating effectively with patients about unusual dosage regimens can reduce adverse events. [16] Clinicians should encourage feedback to ensure that the patient understands the weekly dosage schedule and that the medication should not be used "as needed" for symptom control. Patients should be given clear written instructions that name a specific day of the week for taking the drug, that emphasize the weekly-not daily-dosage schedule, and that explain the possible outcomes of a dosage error. Furthermore, to reduce the medication errors patients may be given a treatment diary to monitor their methotrexate treatment. [16] Pharmaceutical companies should develop new packaging (once weekly package). Another problem with methotrexate is similarity between 2.5mg and 10 mg tablets. Having different color, size and shape for two different strengths can prevent potential confusion. [16] References
Copyright 2008 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv08205f1.jpg] [dv08205f2.jpg] |
| |||||||||

{kind=link}
{kind=link}