 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
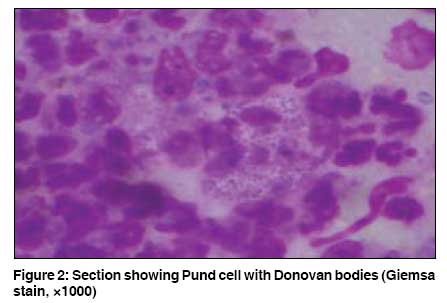
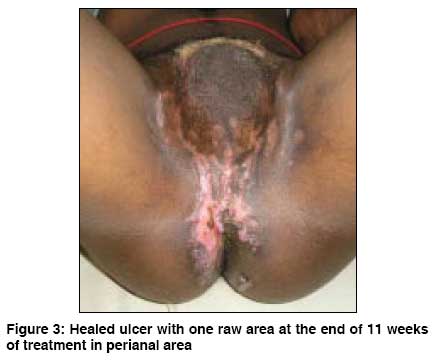
Indian Journal of Dermatology, Venereology and Leprology, Vol. 74, No. 5, September-October, 2008, pp. 490-492 Case Report Donovanosis with auto-amputation of penis in a HIV-2 infected person Chandra Gupta TS, Rayudu Thrimurthulu, Murthy SrinivasaV Department of STD, Rangaraya Medical College, Government General Hospital, Kakinada, Andhra Pradesh Code Number: dv09208 Abstract Donovanosis is a slowly progressive, granulomatous ulcerative disease , caused by Klebsiella (Calymmatobacterium) granulomatis. The disease is known to persist for years together, leading to complications. A male patient aged 30 years with underlying HIV-2 infection presented to the department of STD with painful ulceration over the genital region of 5 months duration, with absence of penis. Tissue smear from the ulcer and histopathological examination revealed large histiocytes with intracellular Donovan bodies (Pund cell). A final diagnosis of donovanosis with auto-amputation of penis with HIV-2 infection was made. The old conventional medicines, viz. streptomycin, doxycycline and amoxycillin, were effective. Though HIV-2 infections are milder than HIV-1 infections in all aspects, donovanosis in this HIV-2 infected case presented with complications. However, since the CD4 count was 748 cells/cmm, the severity is attributed to the long standing nature and negligence by the patient, and not to possible immunodeficiency.Keywords: CD4 count, Donovanosis, HIV-2, Klebsiella (Calymmatobacterium) granulomatis, Pseudocarcinomatous hyperplasia, Pund cell Introduction Donovanosis is a chronic slowly progressive, mildly contagious disease of venereal origin, characterized by granulomatous ulceration of the genitalia and neighboring sites, with little or no tendency to spontaneous healing. [1] It is caused by Klebsiella (Calymmatobacterium) granulomatis, a Gram negative encapsulated rod. The organism was first described by Donovan in 1905 in Madras. [2] It occurs more commonly in tropics, twice as frequently in men as in women, and in those aged 20-45 years. The incubation period varies from 5 days to 5 months. The ulcers are known to persist for years together, leading to complications like pseudo-esthiomene, keloidal or atrophic scarring and consequent strictures and fistulae, and squamous cell carcinoma. Partial or total amputation of penis is one of the rare complications of the disease. One such case of donovanosis with auto-amputation of penis with coexistence of HIV - 2 infection is reported here.Case Report A 30 year old, HIV-2 infected male patient, driver by occupation, presented to our outpatient department, in November - 2005 with painful ulceration over the genital region of 5 months duration, with absence of penis. History of foul smelling discharge and bleeding was present. There was history of gradual, significant weight loss but no fever or diarrhea. He was married and an alcoholic. He gave history of multiple protected and unprotected premarital and extramarital sexual exposures. He had developed an ulcer on the penis 6 years back and which he neglected leading to partial amputation of penis 5 years back. He appeared ill nourished, pale and had generalized lymphadenopathy. Genital examination revealed a large raised irregular, granulomatous ulcer measuring 10 x 9 cm over the pubic, suprapubic and penile area extending on to the scrotum [Figure - 1]. The ulcer floor was red in color with seropurulent foul smelling discharge, bleeding points and necrosis at some places. Multiple smaller ulcers of varying sizes were present in both crural areas extending on to the perineal, perianal areas and buttocks. Penis was absent but a semblance of bud like projection at the penile area was seen. The ulcers were tender but non-indurated. Bilateral, discrete, firm, non-tender inguinal lymphadenopathy was present. Blood investigations revealed hemoglobin of 9gm%. VDRL and TPHA were non-reactive. HIV - 2 was positive (VCCTC, Kakinada, 1999). The CD4 count was 748 cells/ cmm of blood. Giemsa staining of tissue smear revealed presence of large mononuclear cells with Donovan bodies [Figure - 2]. FNAC of inguinal lymph nodes was suggestive of non-specific reactive lymphadenitis. Biopsy sections showed irregular acanthosis with pseudo-carcinomatous hyperplasia and dense collection of polymorphs, large histiocytes, plasma cells and a few lymphocytes in the dermis. The histiocytes had a clear cytoplasm with typical intracellular bodies (cell of Pund and Greenblatt), suggestive of donovanosis. Thus, a final diagnosis of donovanosis with amputation of penis with HIV-2 infection was made. The patient was initially treated with oral metronidazole 400mg 1 TID for 7 days (to take care of anaerobic superinfection) followed by inj. streptomycin 1gm intramuscularly twice daily for 30 days. This was combined with oral amoxicillin 500 mg TID for 17 days, and followed up with doxycycline 100 mg BID for 35 days till he was discharged, at request. Discussion Donovanosis was first recognized in India by McLeod (1882). The disease is endemic in the States of Madras (presently Tamil Nadu and Andhra Pradesh) and Orissa. [1] According to a study conducted by Rama Rao et al , at Kakinada in 1966, donovanosis accounted for 6.1% of total male VD cases and 6.9% of total female VD cases. [3],[4] But another study conducted again at Kakinada by Chandragupta et al . in 2000 -2005 revealed a decreasing incidence from 0.22% (11 cases) in 2000-2002 to 0.01 %(1 case) in 2003-2005. [5] The present case was the only case of donovanosis reported during 2003-2005 in the above said study, signifying rarity of occurrence. Donovanosis usually begins as a papule or a subcutaneous nodule. Nodules erode to form sharply defined, elevated, painless granulomatous ulcers with red beefy granulation tissue which bleed readily on touch. The disease spreads by direct continuity or auto - inoculation of apposing surfaces and may advance onto the lower abdomen and thighs. The present case fits into the abovesaid clinical description. In donovanosis, there is absence of lymphadenopathy even in long standing cases. On the contrary, the present patient had bilateral inguinal lymphadenopathy. The other causes of lymphadenopathy like associated syphilitic infection and malignancy were ruled out by relevant investigations. Fine needle aspiration cytology of a lymph node revealed reactive lymphadenopathy. Thus lymphadenopathy was considered to be due to the associated HIV infection. The disease has a predilection for moist stratified epithelium. This is exemplified in the present case by intact urethral orifice, (lined by columnar epithelium) with normal micturition. The diagnosis of donovanosis is made clinically and confirmed by tissue smear and histopathological examination. The pathognomonic cell found in tissue scrapings is a large (25-90 microns) monocyte containing typical intracytoplasmic bodies (Donovan bodies) which were found in the present case. The ulcers in donovanosis are known to persist for years together, leading to complications such as pseudo-elephantiasis of the genitalia, stenosis of urethral, vaginal and anal orifices, adhesion and / or incarceration of penis into the skin of scrotum, partial or total amputation of penis and squamous cell carcinoma. [1] Our patient had amputation of penis. Here the authors wish to use the term "auto-amputation" of penis to imply the self destructive nature of the disease. Several therapies are reported to be useful for donovanosis. Azithromycin 1g stat followed by weekly doses is effective. Cotrimoxazole, ciprofloxacin, doxycycline or gentamicin are suggested for a duration of 3 weeks or till the ulcers heal completely. [6] In our case, the medicines were used for 11 weeks i.e., till the ulcers almost healed. Azithromycin was not used because of non-availability in our hospital. The combination of streptomycin with amoxycillin and followed by doxycycline was very effective. Doxycycline was continued till the ulcers almost healed [Figure - 3]. The complication of auto-amputation of penis could have been a sequel of long standing disease per se or due to underlying HIV-2 infection. There is increased severity of STDs in HIV-1 infected persons due to immunodeficiency. HIV-2 infection is milder than HIV-1 in all aspects. But in this case, donovanosis presented as large ulceration with auto-amputation of penis. Thus the severity of STDs could probably be no less with HIV 2 infection. However, as the CD4 count was 748 cells/cmm, we attribute the severity of the disease to patient′s negligence rather than to HIV 2 infection. Further observations may throw more light on the behavior of STDs in HIV-2 infections. References
Copyright 2008 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv08208f1.jpg] [dv08208f2.jpg] [dv08208f3.jpg] |
| |||||||||


{kind=link}
{kind=link}
{kind=link}