 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
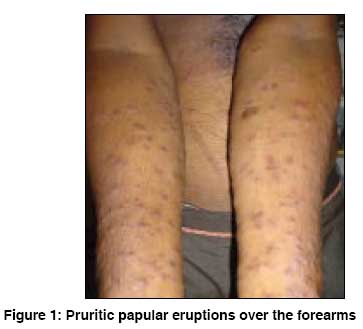
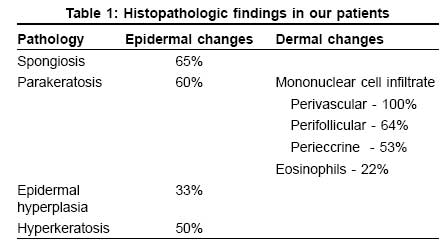
Indian Journal of Dermatology, Venereology and Leprology, Vol. 74, No. 5, September-October, 2008, pp. 501-503 Letter To Editor Pruritic papular eruptions of HIV: A clinicopathologic and therapeutic study Lakshmi SJhansi, Rao GRaghurama, Ramalakshmi, Satyasree, Rao KAnanda, Prasad PGuru, Kumar YHari Kishan Department of Dermatology, Andhra Medical College, Visakhapatnam, Andhra Pradesh Code Number: dv08218 Sir, Pruritic papular eruptions (PPEs) of HIV disease are characterized by chronic, sterile pruritic papules and pustules on the extensor surfaces of the arms, dorsa of the hands, trunk, and face with sparing of the palms and soles. The condition tends to wax and wane. [1] In majority of the cases, the eruptions appear in the advanced immunosuppressive stage of the disease, [2],[3],[4],[5] but eruptions may appear as an initial cutaneous disease of the HIV, with high CD4 lymphocyte count. [6],[7] PPE remains the most common cutaneous manifestation in HIV disease, with prevalence varying between 11% and 46% according to the geographic area; and it is more prevalent in less developed countries of the world. Varying therapeutic successes have been achieved with ultraviolet B rays, antihistamines, pentoxyphylline, and potent corticosteroids. There is no clear consensus on the etiology of PPE, the exact spectrum of this condition, the pathological findings, or the treatment. [1] The present study was undertaken to observe the clinical spectrum and histopathological features of this unique eruption, and its response to various therapeutic modalities. Our study included 30 HIV-positive patients - 17 males and 13 females, with chronic persistent PPE of symmetrical distribution without any definable cause [Figure - 1]. Their age group was 20 to 40 years. Patients with opportunistic infections and systemic diseases were not included. The mean duration of HIV disease was 3.5 years; and of these eruptions, about 6.5 months. Their mean CD4 count was 153 cells/cu. mm. Serological tests for syphilis were negative, and all other routine investigations were within normal limits. From fresh pruritic papular lesions, 4-mm punch biopsies were taken, and the histopathological findings are given in [Table - 1]. The predominant histopathological features were spongiosis, parakeratosis with perivascular mononuclear cell infiltrate. Eosinophilic infiltrate was seen in only 22% of the cases. For treatment purpose, these patients were divided into groups A, B, and C, with each group comprising 10 patients. Patients in group A were treated with dapsone 100 mg daily; group B, with pentoxyphilline 400 mg b.i.d.; and group C, with antihistamines and topical clobetasol propionate cream. For all these groups, treatment was given for 8 weeks and followed-up for up to 6 weeks after stopping the treatment. Antiretroviral therapy was not initiated during this period. In our study, group B patients treated with pentoxyphilline responded faster and remission lasted for longer periods in comparison with patients in groups A and C, but compliance with pentoxyphilline was poor. PPE closely mimics another dermatological entity, viz., eosinophilic folliculitis (EF). In EF, follicular erythematous papules and pustules are seen over the face and central trunk with sparing of acral sites. The lesions are pruritic and chronic but may display periods of improvement, unlike PPE. Histopathology is an important tool in differentiating PPE from EF and many other conditions that can mimic it. [3],[8],[9] In EF, sterile inflammatory infiltrate consists of perifollicular eosinophils; unlike in PPE, which shows perivascular mononuclear cell infiltrate. The etiology of PPE is unclear, although inappropriate response to an exogenous agent such as arthropod may underline the pathogenesis. [10] Some researchers reported PPE to have good response to antiretroviral therapy, and they have suggested that PPE be added to the list of conditions qualifying for specific therapy. [1] Our study reveals that the PPEs of HIV disease are unique clinical eruptions and good clinical indicators of advancing immune suppression. Therefore, early identification and management of these eruptions constitute an important aspect of overall management of HIV disease. References
Copyright 2008 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv08218f1.jpg] [dv08218t1.jpg] |
| |||||||||

{kind=link}
{kind=link}