 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
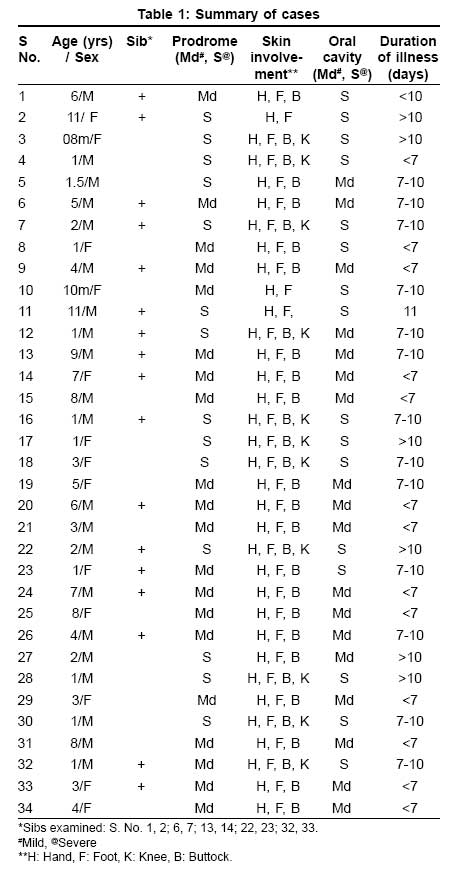
Indian Journal of Dermatology, Venereology and Leprology, Vol. 74, No. 5, September-October, 2008, pp. 503-505 Letter To Editor Hand foot and mouth disease: Emerging epidemics Arora Sandeep, Arora Gulhima, Tewari Vanmalini Skin Department, 5 Armed Forces Hospital C/O 99 APO Code Number: dv08219 Sir, The case report by Saoji VA about hand, foot and mouth disease in Nagpur, made very interesting reading. [1] We in Jorhat district of the state of Assam, India, also witnessed and managed an outbreak of hand foot mouth disease (HFMD). However, our observations differed in various respects from the above case report. We observed a sudden increase in referrals and direct presentation of children in the month of August and September 2007, with undiagnosed discrete, tender, non-itchy vesicular eruption over palms, soles, and buttocks; as well as oral erosions. A total of 34 children fully immunized for their age presented with the above complaints over a 4-week period. Boys accounted for 21 and girls for 13 of the total cases [Table - 1]. The age of the children varied from 8 months to 11 years. Although a large number of children were less than 1 year of age (11 cases), we also had 3 children older than 10 years of age, which is uncommon. [2] Among the affected population, 27 children had a sibling staying with them. Of these, 12 were affected, though we could examine only 5 during their affliction. All children reported within 48 hours of the onset of the eruption. Twelve children less than 3 years of age, as well as 2 children aged 11 years, were more severely affected with a severe prodrome of constitutional symptoms, varying from a febrile illness associated with malaise, irritability, drooling of saliva, and refusal of feeds. These children seemed to have a longer duration of illness and a more severe oral involvement. On examination the lesions consisted of multiple discrete vesicobullous lesions on an erythematous base affecting the hands, feet, knees, and buttocks [Figure - 1]. Oral involvement consisted of aphthous-like ulcers with sparing of other mucosae [Figure - 2]. Older children had more severe oral involvement [Figure - 3], while infants presented with more severe blistering on the skin [Figure - 4]. The skin lesions progressed to form multiple erosions, which healed without scarring. The lesions lasted up to 13 days. Blood counts and Tzanck smears were done in all children. [3] Some smears revealed necrotic keratinocytes, while most revealed inflammatory cells. The cases were diagnosed to be suffering from HFMD after considering a differential diagnosis of varicella, herpes simplex infection, herpangina, aphthous stomatitis, and erythema multiforme. They were managed symptomatically. An active health education campaign, in which the local school authorities were also involved, was also undertaken to pick up early cases. In our study, all cases recovered without any complications or sequelae. There were no fatalities. The outbreak observed by us conformed to the expected seasonal pattern that has been seen in the past. However, the fact that older children were also affected and a tendency for siblings to be involved must alert the physician and probably advocate a follow-up of such cases to prevent serious systemic complications. The panic among parents observed by us also stresses the need for educating the general physician of this entity, which has already been brought out by Saoji [1] in their interesting case report. [1] The first major outbreak of hand, foot, and mouth disease in Sarawak in 1997 marked the beginning of a series of outbreaks in the Asia Pacific region. Some of these outbreaks had unusually high numbers of fatalities, prompting sentinel surveillance for areas endemic for enterovirus-71. [4] Similar sentinel surveillance for coxsackie virus and enterovirus may be warranted in our country to know the epidemiological trends of this disease as there are now increasing number of such cases since they were first reported. [5] References
Copyright 2008 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv08219f4.jpg] [dv08219f2.jpg] [dv08219t1.jpg] [dv08219f3.jpg] [dv08219f1a.jpg] [dv08219f1b.jpg] |
| |||||||||


{kind=link}
{kind=link}
![Figure - 2].](/showimage?dv/photo/dv08219f2.jpg){kind=link}
{kind=link}
{kind=link}