 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
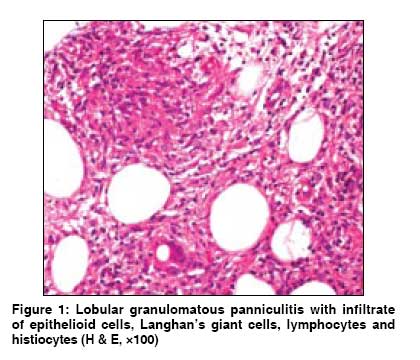
Indian Journal of Dermatology, Venereology and Leprology, Vol. 74, No. 5, September-October, 2008, pp. 505-506 Letter To Editor An atypical presentation of erythema induratum Khandpur Sujay, Sethy PradeepK, Sharma VinodK, Das Prasenjit Department of Dermatology and Venereology, All India Institute of Medical Sciences, New Delhi-110 029 Code Number: dv08220 Sir, Erythema induratum (EI) and erythema nodosum (EN) are diverse entities in the group of panniculitides with distinct clinicopathological features. They have varying etiologies, of which tuberculosis is common to both. In majority of the patients, by meticulous history-taking, cutaneous and systemic examination, a fairly accurate clinical diagnosis can be made, which is further confirmed by histopathology. We present an unusual case of EI that clinically mimicked EN. The diagnosis was confirmed histologically. A 40-year-old woman presented with recurrent crops of erythematous subcutaneous tender nodules on bilateral shins, arms, and forearms since 4 months, each crop subsiding within 2 to 4 weeks, leaving behind hyperpigmentation. It was not associated with constitutional features or systemic complaints. There was no personal or family history of tuberculosis. On examination, she had multiple, discrete, erythematous, tender subcutaneous nodules, 1 to 2 cm in size; and dark- to light-brown post-inflammatory hyperpigmented macules on bilateral shins, extensors of both arms, and forearms. The results of systemic examination were within normal limits. There was no lymphadenopathy, pedal edema, or evidence of erythrocyanotic circulation. We made a clinical diagnosis of EN. Skin biopsy from a leg nodule revealed lobular panniculitis with caseous necrosis, epithelioid cell granulomas, and Langhans giant cells [Figure - 1]. Small vessel vasculitis with extravasation of RBCs, fibrinoid degeneration of vessel wall, and karyorrhexis were also present. The histopathology was consistent with EI. Findings from her hemogram, liver and renal function tests, urine and stool examination, anti-nuclear antibody, anti-streptolysin O titer were within normal limits. Chest x-ray was normal, but findings from Mantoux test was strongly positive (45 mm induration with necrosis). Based on these findings, we initiated four-drug antitubercular therapy (ATT). Within 3 weeks, the lesions resolved and no new lesions appeared. ATT was continued for 6 months. The clinical manifestation of recurrent tender subcutaneous erythematous nodules on extensors of limbs that resolved with hyperpigmentation suggested EN. However, histopathology revealed granulomatous lobular panniculitis with vasculitis, which was consistent with EI. An underlying tubercular focus was suggested by a strongly positive Mantoux reaction and prompt clearance of lesions without any recurrence with ATT. EN and EI are facultative tuberculids in which M. tuberculosis/bovis may be one of the several etiopathogenic factors. They are the most commonly encountered panniculitides in daily practice. In majority of the cases, clinical differentiation between EN and EI is possible. [1],[2] EN is usually bilateral, with lesions developing on shins, knees, and ankles; and occasionally on the face, neck, trunk, arms, and thighs; while EI occurs more commonly on calves on the background of erythrocyanotic circulation. Lesions of EN never ulcerate, and they subside with hyperpigmentation within 3 to 6 weeks, followed by recurrences; while EI nodules usually ulcerate, resolve with atrophic scars, and have a more protracted course. The clinical diagnosis is further supplemented by a characteristic histopathology, which in fully developed EN is a septal panniculitis without vasculitis with fibrosis of septa and mixed inflammatory infiltrate of lymphocytes, histiocytes, multinucleate giant cells, neutrophils and eosinophils, and Miescher′s radial granulomas. Interestingly acute EN may show features of lobular panniculitis or even small- and medium-vessel vasculitis. [3] EI reveals granulomatous lobular panniculitis with or without vasculitis. Atypical forms of EI have been described chiefly in men, including unilateral lesions; lesions involving the shins, thighs, buttocks, arms, and other sites; and those resolving without ulceration. [1] Sanz Vico et al, reported 9 cases of atypical nodular vasculitis in which the clinical presentation included 2 nodules or 1 plaque or lesions that resolved spontaneously without ulceration or scarring. [4] Chew GY et al, described erythematous painful nodules on the thighs and buttock of a 29-year-old woman, mimicking EN clinically, but biopsy revealed lobular granulomatous panniculitis. [5] The lesions cleared within 2 months of ATT. Our patient represented one such atypical variant of EI. Inflammatory nodules occurring on the extremities should also be differentiated from cutaneous polyarteritis nodosa, superficial thrombophlebitis, subcutaneous sarcoidosis, and lymphoma. [1] Niemi et al, described a group of non-definite panniculitis with large, diffuse, indurated subcutaneous plaques without ulceration that healed with scars or pits, and some cases with small acral nodules with or without ulceration. [6] Histology revealed chiefly lobular panniculitis with granulomatous infiltrate and caseation or palisaded granulomas with/without vasculitis and occasionally, only septal panniculitis. Of those who received complete course of ATT, 67% showed no recurrence while lesions reappeared in the remaining cases. None of their EI cases on ATT developed recurrence. The present case was an atypical presentation of EI that clinically mimicked EN. The purpose of this report is to re-emphasize the diverse clinical presentations of EI. References
Copyright 2008 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv08220f1.jpg] |
| |||||||||

{kind=link}