 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
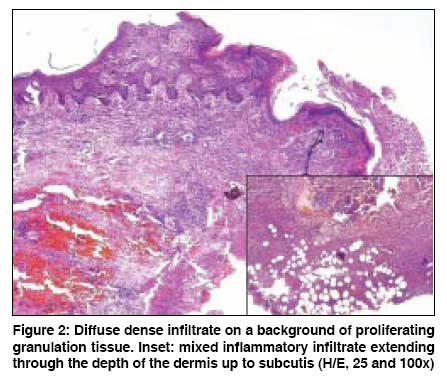
Indian Journal of Dermatology, Venereology and Leprology, Vol. 74, No. 5, September-October, 2008, pp. 506-508 Letter To Editor Pyoderma gangrenosum affecting the vulva Sripathi H, Rao Raghavendra, Prabhu Smitha, Singh Mikki Department of Skin and STD, Kasturba Medical College, Manipal- 576 104 Code Number: dv08221 Sir, Nonvenereal vulvar ulcers often pose a diagnostic and therapeutic challenge to the clinician. Behcet′s disease, Crohn′s disease, pyoderma gangrenosum, premalignant or malignant ulcers, traumatic and factitial ulceration may involve the vulva. A 48-year-old married woman presented with multiple painful ulcers over the genitalia, of 3 months′ duration; and oral aphthae for the past 1 month. Lesions started as erythematous papules rupturing to form painful ulcers with serosanguinous discharge. There was no history of vesiculation, itching, vaginal discharge, joint pain or eye complaints. Findings of general physical examination were unremarkable except for pallor. Genital examination showed large kissing ulcers involving both labia majora and labia minora. Ulcers were tender with undermined edges and indurated base, which were covered with slough and hemorrhagic crusts [Figure - 1]. A few superficial ulcers were present on both thighs, with size varying from 1 to 3 cm in diameter and with undermined edges, and were covered with slough. Bilateral inguinal lymph nodes were enlarged and non-tender. Blood investigations revealed anemia (Hemoglobin- 9.4 g/dL), increased ESR (125 mm/h); and normal blood sugars, renal function, and liver function tests. Serology was negative for human immunodeficiency virus and Treponema pallidum (the venereal disease research laboratory test and treponema pallidum hemagglutination assay). Results of pathergy test were negative. Findings of tissue smear were negative, and skin biopsy was inconclusive. E. coli was isolated from the discharge and was found sensitive to amikacin and clavulanate potentiated amoxycillin. The patient was treated for phagedenic ulcers with appropriate antimicrobials covering both aerobic and anaerobic spectrum, along with local care of ulcers. The patient showed initial improvement but came back within a month with increase in size of genital ulcers. At this point, a differential diagnosis of pyoderma gangrenosum was considered and a biopsy was repeated. The patient was started on oral prednisolone 60 mg and dapsone 100 mg/d. On tapering prednisolone to 40 mg, recurrence was seen. The second biopsy showed features consistent with pyoderma gangrenosum [Figure - 2]. Hence the patient was started on intravenous dexamethasone pulse therapy (100 mg in 5% dextrose on 3 consecutive days in a month) and minocycline 100 mg twice daily, following thorough evaluation, including chest X-ray and Mantoux test. With the first two pulses, the patient showed improvement; but on visit for the third pulse, she developed a new ulcer on left labia. Intravenous dexamethasone pulse therapy and oral dapsone were discontinued after the third pulse and the patient was started on oral thalidomide 100 mg twice daily. Lesions started regressing at the end of 1 month; and by the end of 3 months, all the ulcers healed, with post-inflammatory changes [Figure - 3]. Thalidomide was continued for 1 more month and then stopped. On follow-up at the end of 1 year, there was no recurrence of lesions. Pyoderma gangrenosum manifests as painful cutaneous ulceration with undermined edges, violaceous borders, and necrotic tissue at the base . It is associated most commonly with inflammatory bowel disease, rheumatoid arthritis, and hematological malignancies. [1] It is found rarely on the vulva, and very few cases have been described in literature, most of which are associated with underlying disease. [2] In our patient, initial diagnosis of phagedenic ulcer was considered in view of rapidly spreading genital ulcers. However, treatment with antibiotics showed only partial improvement. Behcet′s disease was ruled out as the patient had only one episode of oral aphthae, negative pathergy test, and absence of systemic complaints. Treatment of pyoderma gangrenosum is challenging, and steroids are the mainstay of treatment, both oral as well as pulse therapy. [3] In recalcitrant cases, other modalities like sulfasalazine, sulfapyridine, dapsone, clofazimine, minocycline, and immunosuppressive agents - azathioprine and cyclophosphamide, mycophenolate mofetil, infliximab, and thalidomide, or plasma exchange, intravenous immunoglobulin, hyperbaric O 2 therapy, nicotine, and potassium iodide are advocated. [4] Hecker et al. treated a case of recalcitrant pyoderma gangrenosum using thalidomide. [5] Effect of thalidomide is immunosuppressive, as well as selectively inhibitory of tumor necrosis factor-alpha (TNF-a). It also inhibits chemotaxis of polymorphonuclear cells. Given the patient′s history of repeated therapeutic failures, thalidomide was started and the patient showed good improvement. References
Copyright 2008 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv08221f2.jpg] [dv08221f1.jpg] [dv08221f3.jpg] |
| |||||||||


{kind=link}
{kind=link}
{kind=link}