 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
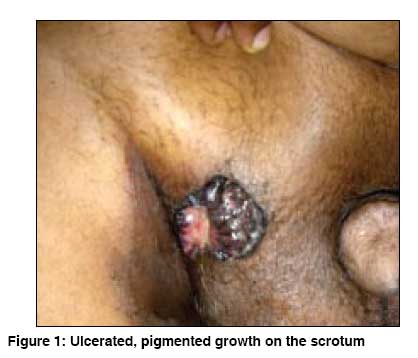
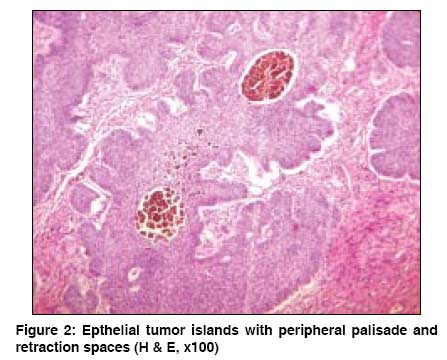
Indian Journal of Dermatology, Venereology and Leprology, Vol. 74, No. 5, September-October, 2008, pp. 508-509 Letter To Editor Pigmented basal cell carcinoma of the scrotum: An unusual site Rao GRaghurama, Amareswar A, Kumar YHari Kishan, Prasad TS, Rao NRamkoteswar Surya Skin Care and Research Center, Visakhapatnam Code Number: dv08222 Sir, The commonest site of basal cell carcinoma is the face; 80% arise above a line from the corner of the mouth to the ear lobe. Occurrence of basal cell carcinoma (BCC) on the scrotum is extremely rare, accounting for less than 0.05% to 0.19% of all BCC cases. [1],[2],[3] Very few cases of BCC on the pudendum have been reported in the literature. [1],[2],[3],[4],[5] We report a case of BCC of the scrotum in a 75-year-old man. A 75-year-old man, a retired civil engineer, presented with a painless, ulcerated, pigmented, and irregularly shaped growth on the right upper aspect of the scrotum, of 2 years′ duration [Figure - 1]. The growth had started 2 years ago as a small asymptomatic pigmented nodule, and it attained the present form during these 2 years. There was no history of exposure to ionizing radiation, chemotherapy, immunosuppressive medications, coal tar, arsenic, or other carcinogens. No prior lymphoma or other malignancy or trauma to the area was present. There was no family history of skin tumors. On examination, there was a single, pigmented, ulcerated growth measuring 4x3 cm over the right upper aspect of the scrotum [Figure - 1]. The growth was non-tender, freely mobile, and not fixed to the underlying structures. There was no regional lymphadenopathy. The penis was normal without any growths or ulcers on it. Both the testes were normal. There were no palpable swellings in the scrotal sac. Abdomen was soft and no palpable masses were felt. All other systems were normal. A provisional diagnosis of ulcerated sebaceous cyst, squamous cell carcinoma, or melanoma was made and the case was investigated. Results of all the routine hematological and biochemical investigations were within normal limits. X-ray chest and ultrasound abdomen revealed no abnormalities. The tumor was excised and sent for histopathological examination. Histopathology revealed pigmented basal cell carcinoma with cells arranged in solid nests with central stellate and peripheral palisaded pattern. Some of the cellular nests showed melanin pigment deposits. Tumor extended from epidermis to deeper dermis. Lateral and deeper resected margins were free from the tumor [Figure - 2]. Postoperative period was uneventful. No recurrence of tumor and lymphadenopathy was observed during the follow-up period of 3 months after the excision of the tumor. The patient was educated about the aggressive nature of BCC of pudendum and was advised to come for follow-up every 6 months for at least 2 to 3 years. Basal cell carcinoma is one of the most common but least dangerous of all cutaneous malignancies. It occurs commonly only on the skin exposed to ultraviolet light and not on mucosal surface. It is a locally invasive carcinoma with no lymphatic spread, but it rarely metastasizes. However, pudendal BCCs behave aggressively and seem to metastasize widely. Pudendal BCC has a predilection for the scrotum in males and labia majora in females. [1] Although ultraviolet radiation may be an important etiologic factor for BCCs on sun-exposed areas, the cause of their occurrence on areas not exposed to sun has not been identified. Chronic skin irritation, previous trauma, exposure to ionizing radiation, coal tar and other carcinogens or immunosuppressive drugs may be responsible for the development of tumors at uncommon sites. [1],[2] In our case, advancing age may be responsible for the rare occurrence of BCC over the scrotum. In view of the aggressive nature of scrotal basal cell carcinoma, all the patients should be kept under surveillance for metastasis for 2 to 5 years after excision of the tumor. References
Copyright 2008 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv08222f2.jpg] [dv08222f1.jpg] |
| |||||||||

{kind=link}
{kind=link}