 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
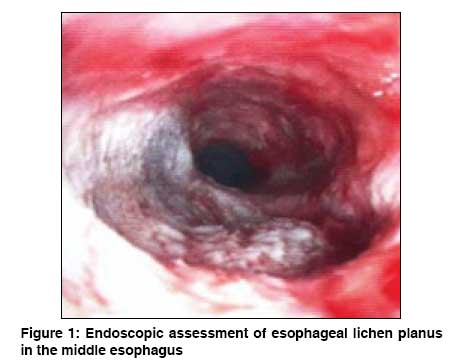
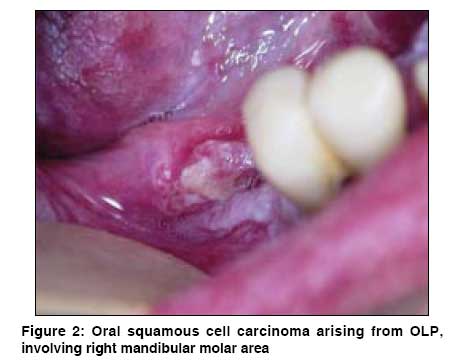
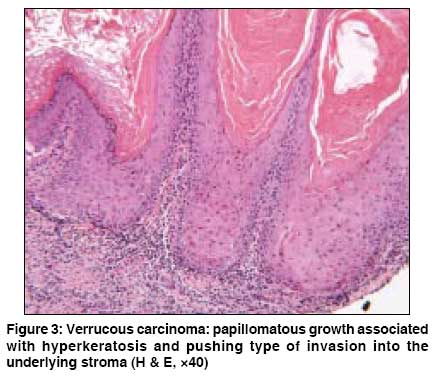
Indian Journal of Dermatology, Venereology and Leprology, Vol. 74, No. 5, September-October, 2008, pp. 509-511 Letter To Editor Oral-esophageal lichen planus associated with oral squamous cell carcinoma Bombeccari GP, Pallotti F, Guzzi G, Spadari F Institute of Dentistry, Department of Oral Pathology and Medicine, University of Milan, Milan Code Number: dv08223 Sir, Oral lichen planus (OLP) is a chronic inflammatory mucocutaneous condition which affects approximately 0.2% to 3.8% of the general population, being more frequent in females. [1] Among OLP cases, only 1% may involve the esophagus. [2] The rate of malignant transformation in OLP is about 0.4% to 1.74%. [3] In May 2004, a 64-year-old Italian woman was referred to our hospital with a history of oral white lesions. Clinical examination showed OLP in her oral cavity with reticular and plaque variants. Bilateral buccal mucosae were affected, particularly on the right side, with evidence of atrophic erosive foci. There were no cutaneous or genital lesions. She had had a sub-total thyroidectomy and suffered from mild hypertension; however, she was not under any medication. The patient was negative for antibodies to HbsAg and hepatitis C virus. Because of oral lesion extensions accompanied by dysphagia, we performed an endoscopy of the pharynx-esophageal tract. The finding of ulcerative esophagitis necessitated an endoscopic ultrasonography, but there was no evidence of malignancy [Figure - 1]. The results of the oral biopsy confirmed the diagnosis of OLP associated with low-degree dysplasia. Therefore, the OLP lesion was subsequently partially removed. We initiated treatment with a topical corticosteroid and the lesions were examined periodically every 3 months, monitoring the upper digestive tract. During a routine follow-up in February 2006, we performed an oral biopsy and took multiple samples using the toluidine vital staining method. The histopathological report showed a focal severe-degree dysplasia in the right retromolar trigonal region, which was promptly removed. In May 2006 a new biopsy revealed an oral squamous cell carcinoma (OSCC) on the sublingual area [Figure - 2]. The radical removal was carried out after a grade 1 neoplasia staging (according to TNM classification) [Figure - 3]. We strongly support the multidisciplinary approach when OLP is associated with esophageal involvement. An esophageal stricture is found in half of these patients, and exceptionally, a squamous cell carcinoma can develop within esophageal lichen planus. [4] It is important to note that within 2 years of follow-up on diagnosis of OSCC, about 10% of the patients develop a new neoplasia in the gastric-respiratory tract. [5] Our case emphasizes that where OLP affects wide areas, multiple biopsy samples and the toluidine vital staining method should be routinely used to assist in the choice of biopsy sites. Such procedures allow us to select the lesion areas more likely to develop a malignant process. With an early diagnosis during the process of carcinogenesis, we can improve survival rates for patients with oral cancer. References
Copyright 2008 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv08223f3.jpg] [dv08223f1.jpg] [dv08223f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}