 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
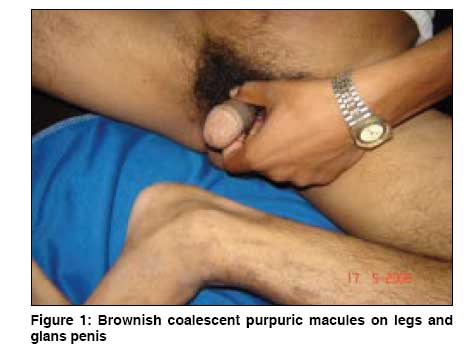
Indian Journal of Dermatology, Venereology and Leprology, Vol. 74, No. 5, September-October, 2008, pp. 516-518 Letter To Editor Schamberg's disease: Involvement of the genitalia Gangopadhyay Asok, Das JayantaKumar, Sengupta Sujata Department of Dermatology, R.K.M. Seva Pratisthan and V.I.M.S., Kolkata Code Number: dv08228 Sir, Schamberg′s disease (SD), (progressive pigmentary dermatosis), is of uncertain etiology. [1] Irregular patches of brown pigmentation due to hemosiderin deposits, with characteristic ′cayenne pepper′ spots, are clinically seen. Though most frequent on the lower limbs, they may occur anywhere in the body, including the palms. [2] To the best of our knowledge, this is the first case of SD involving the genitalia. A 21-year-old bachelor, a shop owner, reported to our OPD with a 3-year history of progressive asymptomatic red-brown lesions scattered over the dorsa of feet, ankles, and distal two thirds of the legs. A year later, similar lesions appeared over the glans penis [Figure - 1]. Circumcised during childhood, there was no history of any medications, local trauma, infection, sexual contact, genital ulcers, or a familial occurrence of similar disorders. The skin lesions in the legs and genitalia were similar, with grouped pinhead-sized coalescent purpuric macules with the typical ′cayenne pepper′ spots in the center and edges. The penile shaft and scrotum were not affected. The patient had a thin build, and there was no pedal edema, varicose veins, regional lymphadenopathy, or systemic abnormality. Routine hematology, biochemistry, and the coagulation profile yielded normal results. A Doppler study of peripheral veins was normal. Hematoxylin and eosin-stained sections from the leg showed a slightly hypertrophic epidermis. The dermis showed vascular prominence in some areas with a scattered perivascular infiltrate of mononuclear cells. Histopathology from the glans showed an almost normal epidermis with acanthosis and papillomatosis in some places and a few odd capillaries with a mononuclear infiltrate in the perivascular area. Scanty pigmentary deposits were present in the mid and lower dermis. Pearl′s staining for hemosiderin deposit was positive. The clinical and histological features led to the diagnosis of SD with unusual involvement of the male genitalia. Venous hypertension, exercise, gravitational dependency, capillary fragility, focal infections, and chemical ingestion have all been suggested as etiological factors of SD. [3] However, doppler study of peripheral veins was normal in our patient. The disease began on the legs, as is commonly seen, with a slow proximal extension. However, subsequent involvement of the glans makes this case unique. SD occurring on sites other than legs has been reported on several occasions before this. Harris et al, [4] described a case of SD on the abdomen of a young male and emphasized the need for careful vigilance for progression to purpuric mycosis fungoides. Another report describes 2 cases with SD on the left elbow and right leg. [5] Histology in both patients was compatible with SD. The authors suspected that aspirin use by the patients could have been an etiologic or contributing factor. Though SD is a rare occurrence in children, a review of 13 cases by Torello et al, showed involvement of the upper limb and trunk in 1 and 3 cases respectively. [6] However, none of these studies or reports refer to any cases of involvement of the genitalia by SD. A peculiar quadrantic capillaropathy was described by Higgins and Cox [7] and they proposed pelvic vascular obstruction as the possible mechanism for the rare distribution. But our patient had SD on both legs, in addition, and we have not been able to explain the etiology of capillaropathy on the genitalia in the same light. No triggering factor for vascular damage due to a local cell-mediated immunological event could be elicited. In spite of the clinicopathological resemblance between the genital and limb lesions, we did consider a few other differential diagnoses for pigmented lesions over genitalia, like penile lentiginosis, penile melanoma, and fixed drug reactions. [8],[9] However they were excluded on clinical and histologic grounds. Pigmented purpuric eruptions are quite resistant to treatment. We prescribed topical steroids and oral pentoxifylline, 400 mg thrice daily, for our patient, leading to partial clearance of both leg and glans lesions in 3 months. References
Copyright 2008 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv08228f1.jpg] |
| |||||||||

{kind=link}