 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
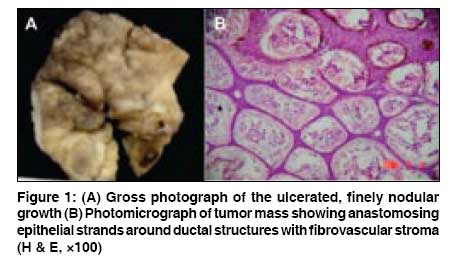
Indian Journal of Dermatology, Venereology and Leprology, Vol. 74, No. 5, September-October, 2008, pp. 518-519 Letter To Editor Solitary eccrine syringofibroadenoma Bothale KalpanaA, Mahore SadhanaD Department of Pathology, NKP Salve Institute of Medical Sciences, Nagpur Code Number: dv08229 Sir, Eccrine syringofibroadenoma (ESFA) is a rare benign proliferation with differentiation towards ductal eccrine structures. It was first described by Mascaro in 1963. [1] It may show variable presentation, ranging from a solitary lesion to multiple papules and nodules arranged in a symmetrical or linear nevoid pattern. The age of onset ranges from 16 to 80 years, but most patients present in the seventh and eighth decades. Distribution of lesions is wide and includes the face, back, abdomen, buttocks, extremities, and rarely the nails. Histopathology of ESFA shows slender anastomosing cords of epithelial cells with or without lumina embedded in a loose fibrovascular stroma. The epithelial cells may show ductal differentiation, often associated with a well-formed cuticle. Approximately 50 cases of ESFA have been reported in the literature till date. [2] An 84-year-old female presented with a slowly growing multinodular lesion on the plantar aspect of foot since 3 years. The lesion was very small (peanut sized) when the patient first noticed it. It increased slowly to attain the present size (5x5 cm). Initially the overlying skin was intact and developed ulceration two and half years later. There was no history of diabetes mellitus or any other cutaneous lesions. A clinical diagnosis of squamous cell carcinoma was considered. A specimen of ulcerated nodular growth with wide local excision of surrounding lace-like skin was received in our department. It was an ulcerated multinodular growth measuring 5x4.5x1 cm. Multiple variable-sized nodules were present in the growth. The largest nodule measured 1x1 cm. Multiple small nodules were also present. Ulcer measured 2x1.5 cm [Figure 1A]. Sections revealed stratified squamous epithelium. Underlying tumor mass was composed of long, branching, anastomosing thin strands or cords of small cuboidal epithelial cells extending from the epidermis into the dermis. Occasional duct-like lumina lined by cuboidal epithelial cells were present in the epithelial strands. The stroma was loose and fibrovascular [Figure 1B]. Clear cell variant of ESFA was reported by Hu et al. in 2005. They studied the immunohistochemistry of ESFA. Their results suggest dual differentiation towards ductal and secretory portions of the eccrine sweat glands. [3] ESFA may occur as a reactive proliferation associated with other conditions like ulcer of skin, chronic lymphedema, venous stasis, nail trauma, burn scar, nevus sebaceous, bullous pemphigoid, and epidermolysis bullosa. [2],[4] Ichikawa et al, [5] studied ESFA in a patient with burn scar ulcer. The authors came to the conclusion that this variant of ESFA seems to be an eccrine duct hyperplasia developing during the restoration and remodeling of skin structures damaged by trauma or ulcerative lesions. [5] In the literature reviewed, most of the case reports of ESFA are associated with reactive conditions; but in our patient, there apparently was no history of diabetes mellitus or any other reactive condition. Hence ESFA may probably arise as a benign neoplastic proliferation of acrosyringeal cells. We followed our patient for 1 year and 3 months after surgery. There was no evidence of any recurrence. Every diagnosed case of ESFA should be followed in view of risk of developing carcinoma because there are some reports of cases of ESFA with carcinomatous transformation. [6] References
Copyright 2008 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv08229f1.jpg] |
| |||||||||

{kind=link}