 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
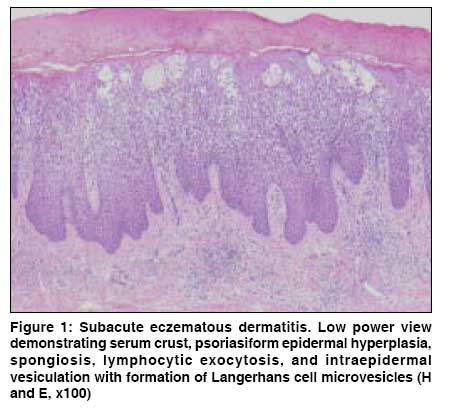
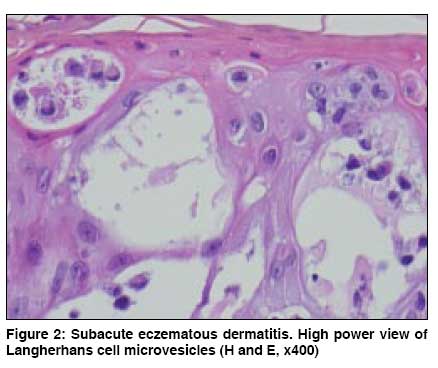
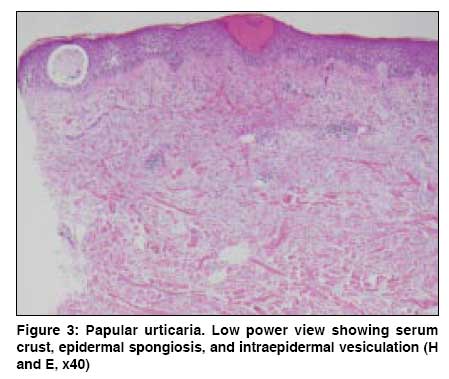
Indian Journal of Dermatology, Venereology and Leprology, Vol. 74, No. 5, September-October, 2008, pp. 523-526 Dermatopathology Deciphering spongiotic dermatitides Gupta Kapil Dermatopathologist, Dermatology Group of the Carolinas, NC Code Number: dv09232 Abstract Clinicians often receive pathology reports proclaiming a spongiotic dermatitis with little in the form of a cogent differential diagnosis. In some cases, this is a natural consequence of the nonspecific nature of the reaction pattern due to matters of sampling error and/or lesional evolution. Further, some conditions are so synonymous in their histologic presentation that to choose one without mention of the other, purely on a histologic basis, may serve to inadvertently mislead the clinician. Despite the often significant histologic overlap amongst the varying spongiotic dermatitides, there are many subtle, yet detectable, features that may serve as clues to the pathogenetic process. Identification and subsequent communication of these features help to narrow the diagnostic possibilities with the ultimate goal of contributing to effective patient management. This article focuses on the histologic details of the spongiotic reaction pattern and presents some of the more common variations of its manifestation which, in conjunction with ancillary inflammatory elements, may help the histomorphologist to arrive at a more concise list of diagnostic possibilities.Keywords: Spongiotic dermatitis, Eczema, Dermatopathology, Differential diagnosis Introduction Spongiotic dermatitis (SD) is a fairly ubiquitous staple in routine dermatopathology practice. Spongiosis is a term used to describe the appearance of the epidermis imparted by intercellular edema with resultant spaces between keratinocytes, often progressing to intraepidermal vesiculation. The pathophysiologic mechanism of spongiosis remains unknown. It has been proposed that keratinocyte apoptosis induced by T-cells affects transmembrane proteins involved in cell to cell adhesion (cadherins) and that this may be responsible for the development of spongiosis. [1] An increase in hydrostatic pressure is also believed to represent a contributory factor. [2] Additional features of a spongiotic dermatitis include serum crust, lymphocytic exocytosis, and collections of Langerhans cell microvesicles within the epidermis. In some instances, a diagnosis of ′spongiotic dermatitis′, in and of itself, is of great clinical utility, such as in the setting of a hand dermatitis where there exists a clinical differential of psoriasis. However, the categorization of an inflammatory condition merely as a ′spongiotic dermatitis′ is often of little diagnostic value, as in many cases, the spongiotic nature of the dermatitis can be detected at the clinical level. The biopsy in these cases is performed in order to further define the process, be it in the form of atopic eczema, allergic contact dermatitis, a drug eruption, urticarial bullous pemphigoid, or some other form of SD. Although in some cases, due to factors such as sampling error or insufficient lesional evolution, the dermatopathologist is left with little choice but to render a generic diagnosis of ′spongiotic dermatitis.′ However, it has been my experience that in most cases, by way of either form or fortune, it is possible to render a more specific diagnosis, or at the very least a more narrow list of diagnostic possibilities. This serves as the principal motivation for this discussion. When examining a lesion showing spongiosis it is important to note the nature of the scale, the degree of spongiosis, and the associated histologic findings. The following discussion will systematically address the potential diagnoses of the spongiotic reaction pattern. It will be stated at the outset that in examining any spongiotic dermatitis one should always maintain a low diagnostic threshold for fungal disease, as this will not be addressed due to the protean and often indefinable associated histologic features of this condition. The discussion will focus on the more commonly encountered conditions so as to maintain an appropriate relevance to routine clinical practice. Prominent Spongiosis When one encounters lesions with prominent epidermal spongiosis, inference of an SD via examination of the scale is unnecessary. Many conditions are associated with this histologic feature and distinguishing between them requires close examination of the dermal alterations. Prominent spongiosis is a common feature of conditions such as nummular eczema, allergic contact dermatitis, bullous pemphigoid, drug eruptions (including photodermatoses), and arthropod bite reactions. Acute, subacute, and chronic eczematous dermatitis lies along a histologic spectrum in which the degree of epidermal hyperplasia progressively increases and the degree of spongiosis progressively decreases. Perhaps the most commonly encountered form of eczematous dermatitis in a given practice is subacute eczematous dermatitis, heralded by psoriasiform epidermal hyperplasia (an epidermal manifestation of chronicity) with an appreciable degree of spongiosis and lymphocytic exocytosis, accompanied by Langerhans cell microvesicles [Figure - 1] and [Figure - 2]. When, in addition to significant epidermal spongiosis, one encounters tissue eosinophilia, one must consider allergic contact dermatitis, urticarial bullous pemphigoid, and a drug eruption among the foremost considerations. Urticarial bullous pemphigoid is of particular relevance when the eosinophils are largely confined to the more superficial aspect of the dermis. Reliable histologic distinction between urticarial bullous pemphigoid and allergic contact dermatitis is often not possible without direct immunofluorescence testing. Spongiosis overlying dermal eosinophils with the added element of interstitial neutrophils, with or without dermal edema, is often seen in the setting of urticarial eruptions such as papular urticaria [Figure - 3] and [Figure - 4]. Conditions such as scabies and arthropod bite reaction are included in this group. With regard to scabies, the tissue eosinophilia is often intense and there is sometimes an associated element of lymphocytic vasculitis. Arthropod bite reactions often demonstrate a punctum in the form of a prominent spongiotic reaction with epidermal necrolysis and a prominent scale crust. This is further associated with an inflammatory reaction that quite often spans the entirety of the dermis and this feature, in conjunction with the density of the inflammatory infiltrate rich in eosinophils, with or without an associated reactive vasculitis, essentially defines the arthropod bite reaction. In contrast to papular urticaria, conventional urticaria lacks epidermal changes, which stands to reason when one considers the clinical morphology of these lesions. In addition, an associated perivascular lymphocytic reaction that is fairly typical of papular urticaria is usually absent in lesions of conventional urticaria. Urticarial bullous pemphigoid (UBP) should be kept in mind in the setting of spongiotic dermatitis with eosinophils. In contrast to the typical presence of a subepidermal vesicle, intraepidermal vesiculation or subepidermal edema may be found in its stead. However, what is most typical of UBP is the relatively superficial nature of the eosinophilic infiltrate distributed in a horizontal fashion across the superficial aspect of the dermis [Figure - 5]. Intraepidermal eosinophils may also be seen. It must be stressed, however, that DIF is often required to confirm the diagnosis, as conditions such as allergic contact dermatitis and, in some cases, spongiotic drug eruptions may be indistinguishable from UBP on a histologic basis. Minor Spongiosis with Prominent Scale An SD can often be detected even in the presence of little to no spongiosis via examination of the scale. This is often in the form of mounds of parakeratosis and/or the presence of serum crust. If one encounters these as the predominant histologic findings, it is then important to pay close attention to the dermal changes. For instance, mounds of parakeratosis with minor spongiosis overlying a slight superficial perivascular lymphocytic infiltrate with erythrocyte extravasation within the papillary dermis, often accompanied by ′entrapment′ of erythrocytes within the lower aspect of the epidermis, are features characteristic of pityriasis rosea (PR) [Figure - 6]. It is important to note that many cases of PR often harbor eosinophils, and sometimes interface change. The latter, however, should not be very significant and never the predominant finding in the lesion. It is also important to understand that this classic histologic profile of PR can be seen in the setting of alternative eczematous eruptions, including drug reactions. A few conditions that very closely mimic the histopathologic alterations of PR include papular acrodermatitis of childhood (Gianotti-Crosti syndrome), some lesions of guttate psoriasis, drug eruptions, and the superficial variant of erythema annulare centrifugum. It is important to note, in fact, that the typical histologic changes of PR are by no means unique to this condition, as alternative forms of SD, such as pityriasis rosea-like drug eruptions, can show very similar findings. The clinical presentation is, therefore, of significant import. In some cases one encounters a confluent parakeratotic scale, sometimes with mound formation, implying a spongiotic dermatitis; however, with no spongiosis and an almost insignificant degree of perivascular lymphocytic infiltration involving the superficial dermal vasculature. These findings raise diagnostic consideration to small plaque parapsoriasis, a diagnosis that can only be made in the presence of corroborative clinical evidence of digitate lesions. Select Miscellaneous Conditions Of particular clinical significance is the matter of cutaneous T-cell lymphoma, evolving patch stage mycosis fungoides (MF) in particular. In some cases, histologic distinction between evolving MF and other forms of spongiotic dermatitis, perhaps most commonly eczematous eruptions, is as a matter of fact, impossible. This serves as a prime example of the role that sampling error and/or lesional evolution play with regard to histologic diagnosis of clinical dermatoses. Most dermatopathologists will have encountered a biopsy reminiscent of eczema, only to encounter later biopsies of the same patient that demonstrate compelling features of MF. When one encounters a biopsy with psoriasiform epidermal hyperplasia, minimal spongiosis, and lymphocytic exocytosis out of proportion to the degree of spongiosis, overlying dermal fibroplasia ("wiry collagen bundles") with a somewhat band-like lymphocytic infiltrate with preservation of the dermal-epidermal junction, it is important to mention this possibility. This is particularly important when one encounters a biopsy from a patient whose rash is particularly persistent and chronic. The matter of lymphocytic atypia is highly subjective and, in my opinion, overstated. It is also important to note that in many cases, MF and lymphomatoid drug eruptions cannot be distinguished on a histologic or immunohistochemical, or even molecular basis. Therefore, it is always important to be aware of this fact even in those lesions that show typical histologic, and often clinical, morphologic changes of MF. When examining a biopsy that demonstrates some degree of spongiosis and a band-like lymphocytic infiltrate with preservation of the dermal-epidermal junction, with the added features of focal dyskeratosis, an increase in junctional melanocytic frequency, and increased pigment in the mid to upper layers of the epidermis, it is important to raise the possibility of a lichenoid photodermatosis. These conditions are often seen in association with a sensitizing medication and, therefore, dermal eosinophilia is a relatively constant feature. Conclusion Spongiotic dermatitis is a reaction pattern that is seen in association with a variety of dermatologic conditions. Spongiosis, as an individual feature, is insufficient to provide an accurate diagnosis. However, its presence, in association with the coexistent epidermal and dermal changes often provides sufficient evidence for a relatively specific diagnosis or diagnostic category. In this regard, a comprehensive understanding of a lesion′s complete histologic profile will serve to enhance communications with clinicians, with appropriate patient management as the natural intended consequence.References
Copyright 2008 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv08232f3.jpg] [dv08232f4.jpg] [dv08232f6.jpg] [dv08232f5.jpg] [dv08232f1.jpg] [dv08232f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}