 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
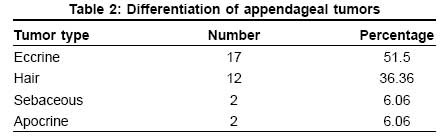
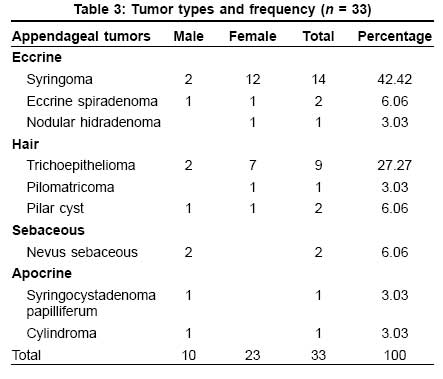
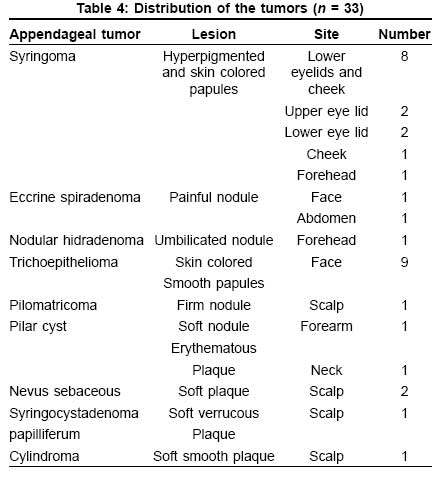
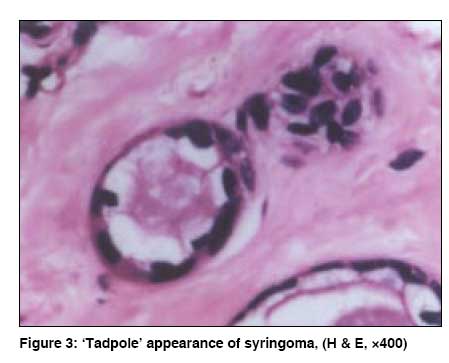
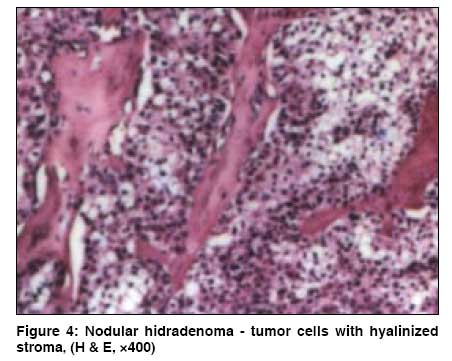
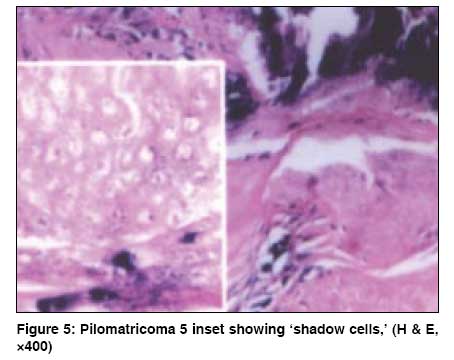
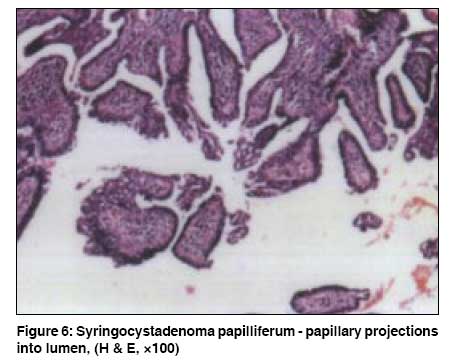
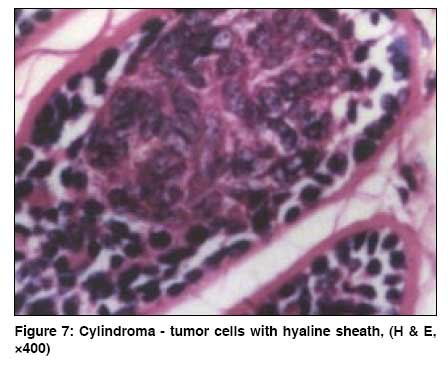
Indian Journal of Dermatology, Venereology and Leprology, Vol. 74, No. 5, September-October, 2008, pp. 550 Net Study A clinicopathologic study of skin appendageal tumors Nair PradeepS Department of Dermatology and Venereology, Medical College Hospital, Trivandrum- 695 011, Kerala Code Number: dv08239 Abstract Background: Appendageal skin tumors belong to a heterogenous group of tumors with specific histopathology. The aim of this study is to determine the pattern of appendageal tumors in skin biopsies done in our department.Methods: This is a 3-year retrospective descriptive study of all patients who were diagnosed to have skin appendageal tumors in our department, and the diagnoses were confirmed by histopathology. The tumors were classified as eccrine, hair, sebaceous, and apocrine after a detailed examination of routine hematoxylin and eosin sections. Results: The total number of cases in the study was 33 - 10 males and 23 females. Tumors with eccrine differentiation constituted the maximum, 17 cases (51.5%); followed by tumors with hair differentiation, 12 cases (36.36%); tumors with sebaceous differentiation, 2 cases (6.06%); and apocrine tumors, 2 cases (6.06%). Syringoma constituted the commonest eccrine tumor, 14 cases (42.42%); while trichoepithelioma was the commonest hair tumor, 9 cases (27.27%). The other eccrine tumors were eccrine spiradenoma, 2 cases (6.06%); and nodular hidradenoma, 1 (3.03%). The other hair tumors were pilar cyst, 2 (6.06%); and pilomatricoma, 1 (3.03%). The sebaceous tumors constituted 2 cases (6.06%) of nevus sebaceous. Syringocystadenoma papilliferum, 1 (3.03%); and cylindroma, 1 (3.03%), constituted the apocrine tumors. Conclusions: Appendageal skin tumors are relatively uncommon. Histopathology is mandatory for the diagnosis. No tumor showed malignant change in this study. Keywords: Appendageal skin tumor, Syringoma, Trichoepithelioma Introduction The skin appendageal tumors (ATs) encompass a wide variety of tumors clinically presenting as papules and nodules and with histologically distinct features. They are basically classified into four groups: tumors with differentiation towards hair follicles, sebaceous glands, eccrine or apocrine glands. [1] These tumors basically originate from undifferentiated pluripotent stem cells and finally differentiate to specific tumors influenced by genetics, local vascularity, and the microenvironment of the epidermis and dermis. [2],[3],[4] These tumors are usually benign, but rarely malignancy can supervene. ATs usually present with papules and nodules. They are usually missed clinically and often confirmed by histopathology. Immunohistochemistry may help in confirmation of the diagnosis. [5] We do occasionally see ATs in our department, diagnosed in most cases following a skin biopsy of an asymptomatic papule or a nodule. There are very few studies in appendageal skin tumors, other than isolated case reports. Keeping these factors in mind, we decided to undertake this study to determine the pattern of ATs in our patients.Methods This is a retrospective descriptive 3-year study done in our. Data was collected after a thorough study of the outpatient, inpatient, and histopathological records. Histopathological diagnosis was mandatory for inclusion in the study. Cases clinically diagnosed as appendageal tumors, but not histologically, were excluded from the study. The histopathology specimens were routine hematoxylin and eosin sections. Following this criterion, the cases selected for the study were then classified into follicular, sebaceous, eccrine, and apocrine tumors. [1] Finally a total of 33 cases were included in this study.Results The total number of patients analyzed in this study was 33, constituting 10 males (30.30%) and 23 females (69.70%). This constitutes about 0.20% of the total new dermatology cases seen in the same study period. The male-female ratio was approximately 1:2.3. The mean duration of illness was 5.31 years; the shortest duration being 2 months and the longest duration being 8 years. The age group distribution is given in [Table - 1]. The age group 11-20 years constituted the maximum number of cases, 9 (27.27%). The differentiation of the tumor types is given in [Table - 2], while the individual tumor types and frequency are given in [Table - 3]. Eccrine tumors were the commonest in this study (17 cases, 51.5%), of which syringoma [Figure - 1] constituted the maximum (14 cases, 42.42%); followed by hair tumors (12 cases, 36.36%), of which trichoepithelioma [Figure - 2] was the commonest (9 cases, 27.27%). The clinical presentation and distribution of the tumors are given in [Table - 4]. Face was the commonest site to be affected (25 cases, 75.75%), followed by the scalp (4 cases, 12.12%).Discussion Only 33 cases seen in a 3-year period indicates that ATs are relatively uncommon. There was a female preponderance in this study. This could be attributed to the fact that syringoma was the commonest tumor seen in this study, and syringoma has a female preponderance. [1] The long mean duration (5.31 years) of the tumors seen in this study, as well as their presentation in most cases as asymptomatic papules and nodules, shows the benign nature of the tumors. The greatest frequency of cases was seen in the young age group (11-20 years), which is in concordance with other studies showing that ATs are disorders of the young. [1],[2],[3] Syringoma was the commonest AT seen in this study and was characterized histologically by the presence of cystic ductal structures lined by 2 layers of cells. Some of the ducts showed a comma-like tail of epithelial cells at one end, giving the appearance of a ′tadpole′ [Figure - 3]. Enzyme histochemical studies show syringoma to be rich in eccrine enzymes like succinic dehydrogenase, phosphorylase, and leucine aminopeptidase. [1] The 2 cases of eccrine spiradenoma seen in this study were painful tumors, as mentioned in literature, and characterized histologically by multiple lobules of tumor epithelial cells separated by a fibrous stroma. [6] The tumor cells were arranged in cordlike structures containing small epithelial cells with dark nuclei in the periphery and large epithelial cells with pale nuclei in the center. However, the hyaline material seen in the stroma, as described in literature, was absent in our cases. [7] The case of nodular hidradenoma was characterized by lobulated tumor masses in the dermis with eosinophilic hyalinized stroma and lumina and cyst [Figure - 4]. The tumor masses showed 2 types of cells. One cell type was rounded or fusiform with round nucleus and basophilic cytoplasm, while the other cell was round with small dark nuclei and clear cytoplasm. The clear cytoplasm is due to deposition of glycogen and hence the alternate terminology, clear cell hidradenoma. [8] Trichoepithelioma was the commonest follicular tumor seen in this study. All the cases in this study were of the multiple type (autosomal dominant) even though positive family history was obtained in only 4 cases. The gene for trichoepithelioma has recently been located to chromosome 9p21. [9] The tumor was characterized by multiple horn cysts and islands of basophilic tumor masses with peripheral palisading of the nuclei. The basaloid cells are hair germinative cells, and the horn cysts are attempts at follicular canal formation. It may be difficult to distinguish between trichoepithelioma and basal cell carcinoma (BCC) histologically. Papillary mesenchymal bodies are fibroblastic aggregates, which represent abortive attempts to form the papillary mesenchyme, are not seen in BCC. The case of pilomatricoma (calcifying epithelioma of Malherbe) was characterized by a sharply demarcated tumor island composed of 2 types of cells, one basophilic with elongated nuclei and the other with eosinophilic cytoplasm and a central unstained area in the region of the nucleus, known as ′shadow cells′ [Figure - 5]. Recent studies show that pilomatricoma shows mutation of the b-catenin gene, which in turn may affect cell-to-cell adhesion. [10] Pilomatricoma may rarely lead to carcinoma, and metastases can occur especially to the lungs. [11],[12] The pilar cyst (trichilemmal cyst) was characterized by a cyst lined by epithelial cells, the peripheral layer of cells showing palisading. Trichilemmal cyst may transform to proliferating trichilemmal cyst, which in turn can lead to malignancy. [13] The 2 cases of nevus sebaceous showed hyperkeratosis, irregular acanthosis, and papillomatosis of the epidermis while the dermis showed numerous mature and partially mature sebaceous glands. Even though other appendageal tumors may develop in a nevus sebaceous, this was not seen in our cases histologically. [14] The case of syringocystadenoma papilliferum showed a cystic invagination with numerous papillary projections in the lower part lined by 2 layers of cells [Figure - 6]. Positive immunoreactivity with gross cystic disease fluid protein-15 (GCDFP-15) is seen, indicating tumor of apocrine origin. [15] Recent studies show loss of heterozygosity at chromosome 9q22 in cases of syringocystadenoma papilliferum. [16] The case of cylindroma was characterized by multiple islands of tumor cells lined at the periphery by small cells with dark nuclei with palisading and the center containing large cells with light staining nuclei. The tumor was surrounded by a hyaline sheath, and there were hyaline droplets found in the tumor islands [Figure - 7]. Rarely, malignant transformation can occur in cylindroma. [17] The early recognition of some ATs is also important as they may be markers of some syndromes associated with internal malignancy, like Cowden′ syndrome. Syringoma and trichoepithelioma may be treated with diathermy, while surgical excision is the treatment of choice for other ATs. None of the cases in this study showed any malignant change histologically. Very few studies in appendageal tumors are available in literature; and in spite of the best of our efforts, we could not find any Indian studies on this topic, except isolated case reports. [18],[19] References
Copyright 2008 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv08239f4.jpg] [dv08239t2.jpg] [dv08239f7.jpg] [dv08239t4.jpg] [dv08239f6.jpg] [dv08239f1.jpg] [dv08239t3.jpg] [dv08239t1.jpg] [dv08239f5.jpg] [dv08239f2.jpg] [dv08239f3.jpg] |
| |||||||||


{kind=link}
{kind=link}
{kind=link}
![Figure - 1]](/showimage?dv/photo/dv08239f1.jpg){kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}