 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
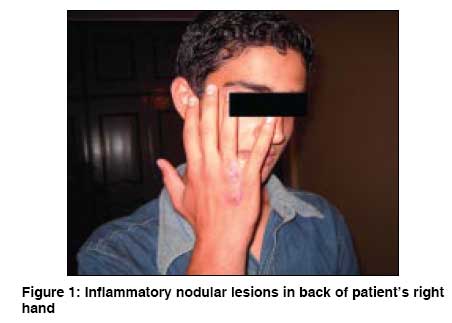
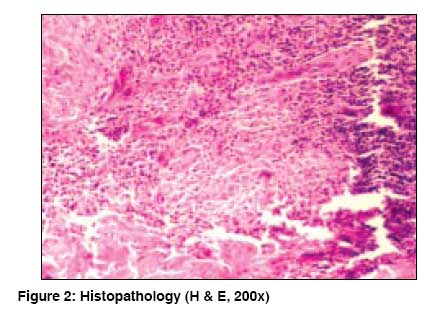
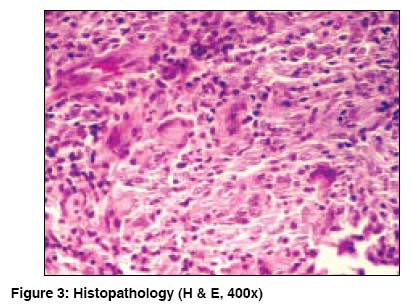
Indian Journal of Dermatology, Venereology and Leprology, Vol. 74, No. 5, September-October, 2008, pp. 551 Net Quiz Nodules and bullae on the back of the hand with axillary spread Golpour M, Ghasemi M Department of Dermatology, Mazandaran University of Medical Sciences, Pasdaran Boulevard, Boo-Ali Hospital, Sari Code Number: dv08242 A 16 year-old aquarium worker presented with nodules and bulls on the back of the right hand since one year. The nodules first appeared on the hand and then over the forearm and the right axilla. The nodules became larger and developed a bulla on top which then ruptured and formed an ulcer [Figure - 1]. The Mantoux test was 22 mm (normal range< 5mm). Chest X-ray was normal. Histopathology of the lesion on hand is shown in [Figure - 2] and [Figure - 3]. What is your Diagnosis ? Diagnosis: Fish tank or swimming pool granulomaThe biopsy showed tuberculoid granuloma with Langhan′s giant cells. Culture from the biopsy material grew Mycobacterium marinum . The diagnosis of fish tank granuloma was based on clinicopathologic correlation and culture. Because, fish tank granuloma with sporotrichoid distribution responds well to rifampicin and ethambutol, [1] these drugs were begun with complete healing of the lesions in 6 months. Discussion Swimming pool granuloma is caused by Mycobacterium marinum . The first report of the infection was in salty water fish in Philadelphia in 1926. Human skin infection was first reported in people swimming in an infected swimming pool in 1951. [2] The present patient was working with aquarium water. The infection is usually limited to the skin, but in a person with immunodeficiency, it may disseminate to sub-mucosal tissue, bone, bursa or joint. [1],[3],[4] Sometimes the lesions are multiple both in normal and immunodeficient subjects. [3] After 2-3 weeks, nodules or plaque could evolve into an ulcer with purulent discharge. The symptoms may vary from asymptomatic to painful dermal nodules. [5] Sometimes, the lesions have sporotrichoid distribution along the lymphatic pathway, [4] a phenomenon observed in our case. Differential diagnosis includes typical skin tuberculosis caused by infected water from swimming pool. Absence of regional adenitis differentiates fish tank granuloma from cat scratch fever and primary inoculation tuberculosis; lymphadenopathy was not observed in our case too. Endemic leishmaniasis or sporotrichosis also shows sporotrichoid pattern of lesion and need to be differentiated. [6] There is no endemic leishmaniasis or sporotrichosis in our region. Other mycobacterial infections such as Mycobacterium kansasii , Mycobacterium chelonie , and Mycobacterium gordonae may also manifest in sporotrichoid pattern. [7] In Edelstein′s series of 31 patients with M. marinum infection, 90% of the lesions were observed on the upper limbs, [8] which was also the case in our patient. The histopathological patterns of fish tank granuloma include: caseous or non-caseous form of dermal granulomas made up of lymphocytes and histiocytes. The organism can be cultured in Lowenstein-Jensen medium at 32-37°C, and are acid fast bacilli. [9] The skin tests using specific antigens against Mycobacterium marinum have low diagnostic value. [10] The Mantoux test is not often helpful. History of working with aquarium water, contact with fish or swimming pool as well as the existence of granuloma in histopathological picture can be helpful in diagnosis. [3] Our case had a history of working with aquarium water, and granuloma in histopathology and positive culture. The treatment includes antibiotics [1] such as minocycline, trimetoprim-sulfamethoxazole, rifampicin, and clarithromycin. Edelstein reported that combination therapy of rifampicin and ethambutol is more effective than minocycline alone. [2],[8] The diagnosis must be re-evaluated in cases resistant to therapy, and if confirmed, excision and debridement should be considered. Infections due to M. marinum are uncommon but not rare. Diagnosis should be confirmed by culture and biopsy as other etiological agents may produce identical lesions. A prolonged course of antibiotic therapy is curative in most superficial cases but adjunctive surgical debridement is often indicated in extensive and deep infections. References
Copyright 2008 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv08242f2.jpg] [dv08242f1.jpg] [dv08242f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}