 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
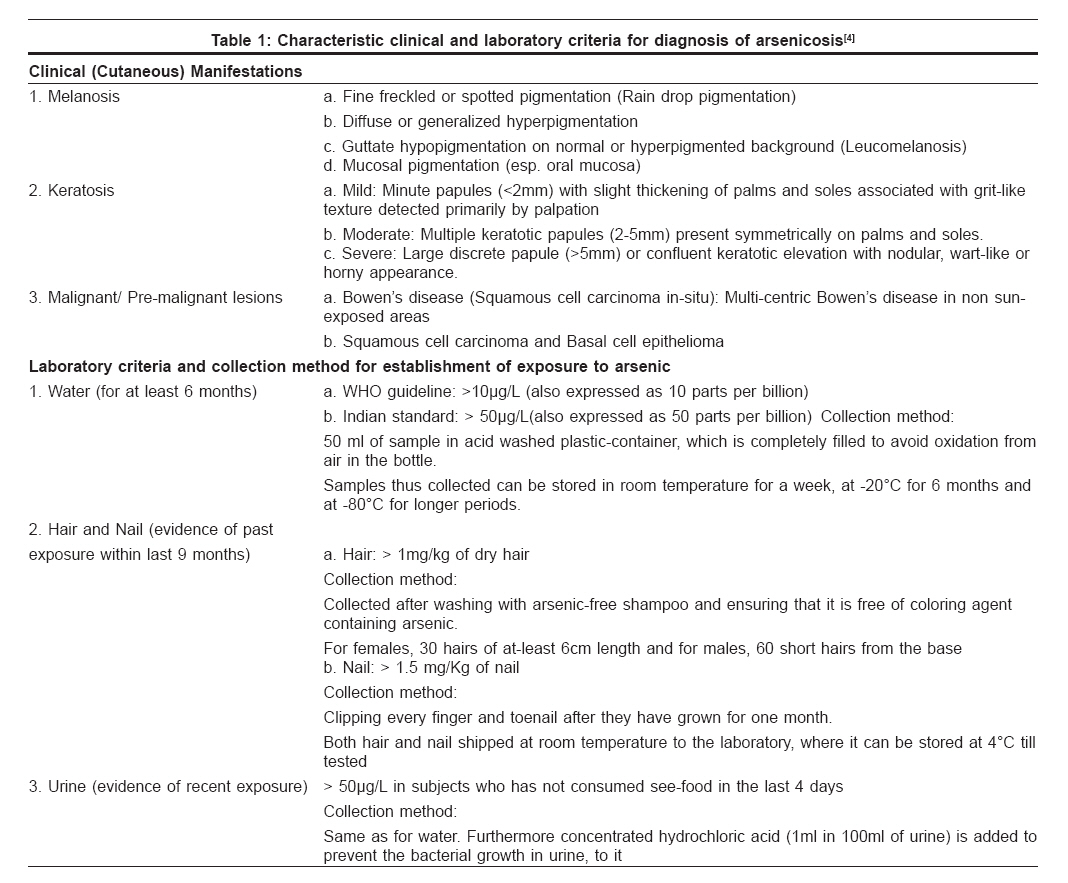
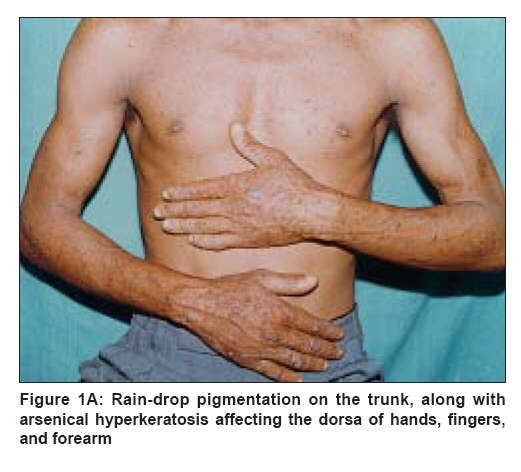
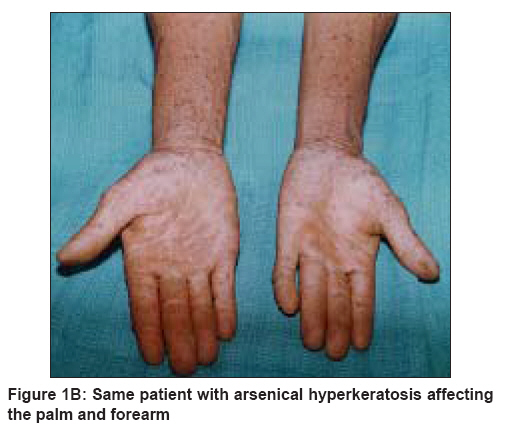
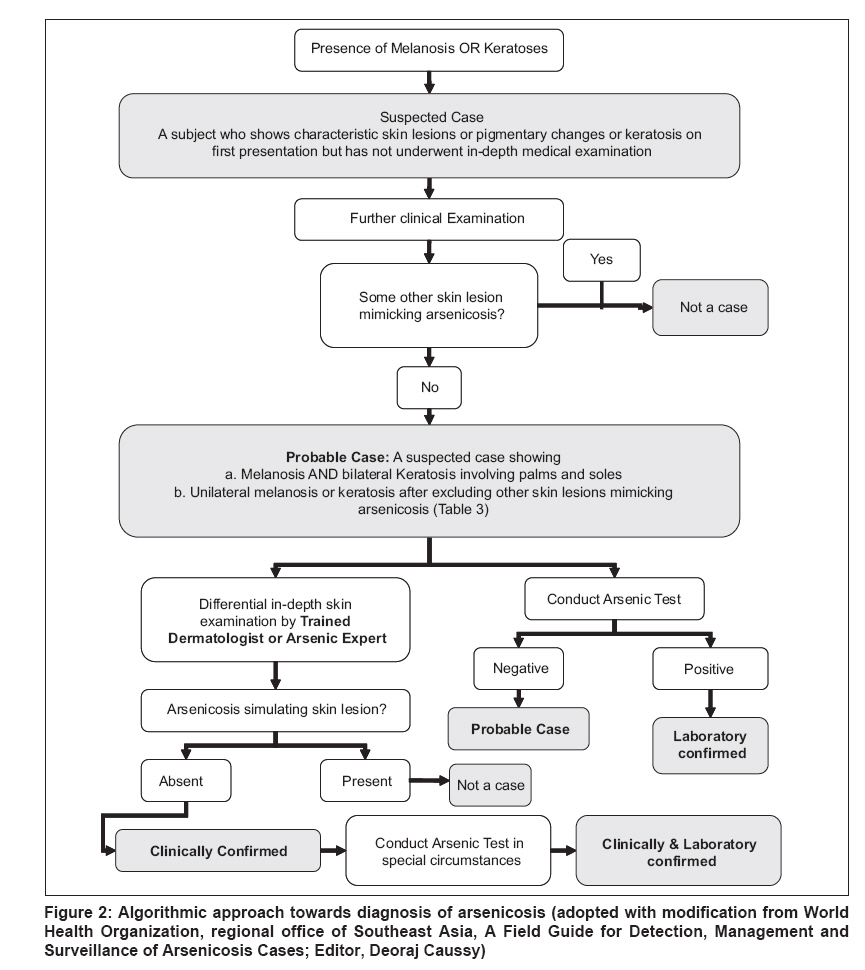
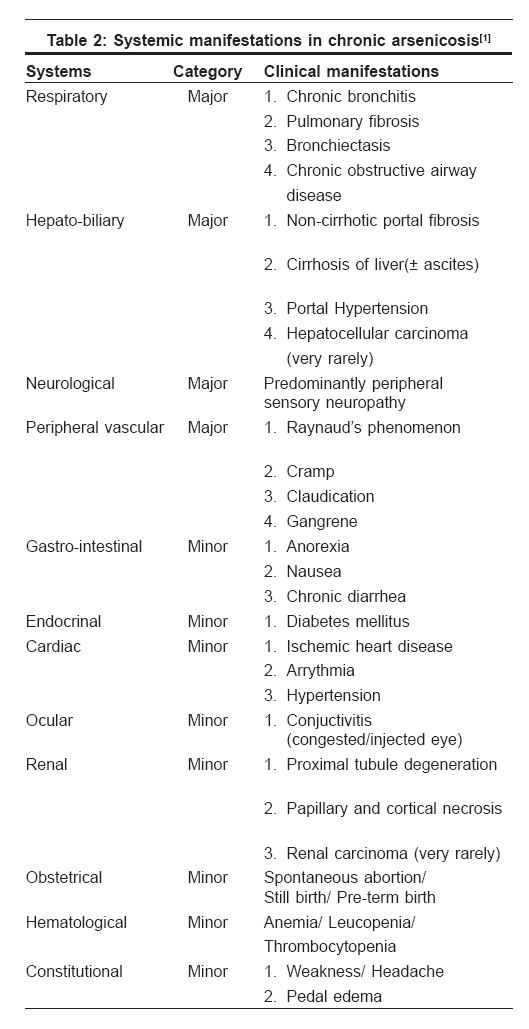
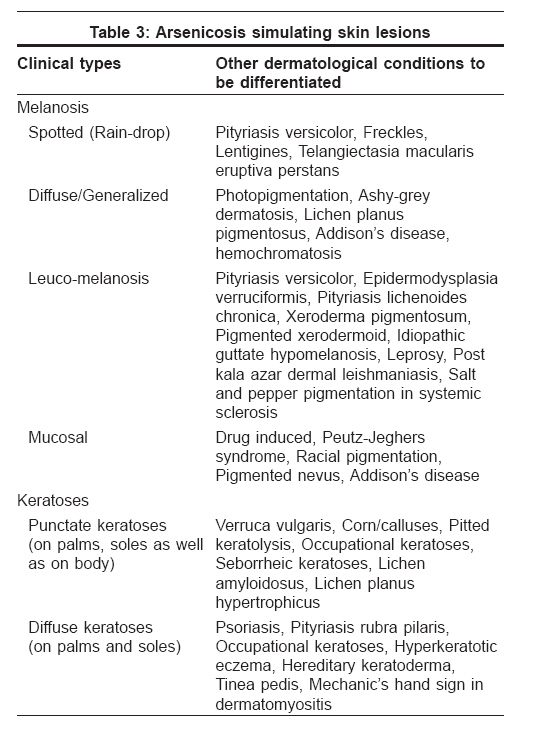
Indian Journal of Dermatology, Venereology and Leprology, Vol. 74, No. 6, November-December, 2008, pp. 571-581 Seminar: Chronic Arsenicosis in India Arsenicosis: Diagnosis and treatment Das NilayKanti, Sengupta SujitRanjan Department of Dermatology, Medical College, Kolkata-700 073 Code Number: dv08246 Abstract Diagnosis of arsenicosis relies on both clinical and laboratory criteria, but principally it can be diagnosed on the basis of its cutaneous manifestations. Cutaneous manifestations (melanosis, keratosis, and cutaneous cancers) are essential clues in the diagnosis, and trained dermatologists or arsenic experts are able to clinically confirm a case even without laboratory backup. Although systemic manifestations are not considered as diagnostic hallmarks, yet their presence serves as important telltale signs in arriving at the diagnosis. In countries where laboratory facilities are available, measuring the level of arsenic in drinking water (consumed in the last 6 months), urine, hair, and nails is of immense value. Newer biomarkers of arsenic exposure are being explored to provide early information about arsenic intoxication, of which urinary porphyrin level, blood metallothionein have shown promising results. Controlling the problem of arsenicosis depends on various factors, of which the most important is cessation of intake of arsenic-contaminated water. Deep wells, traditional dug wells, treatment of surface water, rainwater harvesting, and removing arsenic from the contaminated water by arsenic removal plant or arsenic treatment unit are the available options for providing arsenic-free drinking water. The role of nutrition and antioxidants in preventing the onset of symptoms of arsenicosis is also of importance. Nonspecific therapies (e.g., keratolytics for hyperkeratosis) cannot also be ignored and serve as palliative measures. The persons affected need to be followed up at regular intervals to detect the onset of cancers (if any) at the earliest. Role of counseling and education should never be underestimated since absence of public awareness can undermine all efforts of mitigation measures.Keywords: Arsenicosis, Chronic arsenic ingestion The 20 th century has witnessed an emerging threat to mankind in the form of arsenicosis, which is showing no sign of decline with time and for which, till date, no single effective cure is known. The metalloid arsenic in drinking water on prolonged consumption leads to a multi-system disorder with prominent cutaneous features, with myriads of internal organ involvement, as well as cancers. [1] In the recent years, arsenicosis has emerged as a global public health concern, with the major brunt being born by Asian countries (including Bangladesh, India, and China). [2] This has necessitated the world agencies to undertake immediate mitigation measures to tide over the crisis. The successful mission towards elimination of this health hazard rests on the 3 pillars, viz., diagnosis, prevention, and management. Arsenicosis Case Definition Arsenicosis has been defined by the WHO working group[3] as a "chronic health condition arising from prolonged ingestion (not less than 6 months) of arsenic above a safe dose, usually manifested by characteristic skin lesions, with or without involvement of internal organs."Diagnosis of Arsenicosis Diagnosing a disease with precision is of utmost importance, without which no management effort will be fruitful. Apart from clinical signs and symptoms, laboratory backup is always needed for the confirmation of any diagnosis. At the same time, it is also desired that the diagnostic tools be so designed as to make them uniformly available under the field condition. These issues are to be kept in mind while formulating the criteria for diagnosis of arsenicosis. The clinical and laboratory criteria [Table - 1] are both essential and integral elements for the diagnosis of arsenicosis, but principally it can be diagnosed on the basis of its cutaneous manifestations. [4] It has been suggested that skin lesions are the commonest and earliest manifestation in arsenicosis patients, [5],[6] justifying the emphasis placed on cutaneous lesions in the diagnosis. A thorough physical examination is invaluable as it can reveal the presence of pigmentary and/or keratotic skin changes, which are the hallmarks of the disease [Figure 1A],[Figure 1B]. Among the different cutaneous features, melanosis is found to be the earliest and commonest; [7],[8] whereas keratosis on soles is suggested to be the most sensitive marker for detection of arsenicosis at an early stage. [9] The melanosis may be diffuse or patchy, may take up a rain-drop or leucomelanosis pattern, and at times may produce pigmentation of mucosa. Keratoses can be graded as mild, moderate, or severe depending on the thickness and size of the keratotic lesions (papules, plaques, and nodules). Presence of Bowen′s disease or squamous/basal cell carcinoma also serves as diagnostic clue for arsenicosis. Sudden increase in size, cracks and fissures, bleeding on top of keratotic lesions suggest malignant transformation. WHO′s regional office of Southeast Asia has come up with an algorithmic approach [Figure - 2] to diagnose arsenicosis with locally available resources. [4] This algorithmic approach was shown to have specificity> 80% and sensitivity> 80% and is acceptable for field purpose. There are several non-dermatological conditions which are not highlighted as clinical criteria for diagnosis of arsenicosis but are frequent accompaniment of arsenicosis. They include chronic cough, respiratory distress, hepatomegaly, non-cirrhotic portal fibrosis, cirrhosis, ascites, peripheral neuropathy, peripheral vascular disease, hematuria, non-pitting edema, etc. [Table - 2]. [1] It becomes essential to look for these systemic manifestations since they can at times be of diagnostic importance. The fact that all cases of arsenicosis do not manifest cutaneous features at the very outset is a reason why evaluation of systemic condition should be done to pick up the suspected cases. Residence of the affected person in an endemic zone (as in the Gangetic belt); or similar cutaneous change in persons belonging to the patient′s family or neighborhood who consume water from the same source can be an important diagnostic clue in suspected/probable cases. Differential diagnosis of arsenicosis There are many dermatological mimickers [Table - 3] that can produce either melanosis or keratoses and at times make it difficult for the physician to diagnose. WHO has also highlighted that in the event a patient presents with skin lesions based on which arsenicosis can neither be confirmed nor be ruled out, the case should be considered a ′suspected/probable case′ and referred for reevaluation in 6 to 12 months. [4] Although the manifestations of arsenicosis cannot be limited to cutaneous features, yet for the purpose of case definition, WHO has not yet included the systemic manifestations as diagnostic hallmarks. Laboratory support in diagnosis of arsenicosis Laboratory tools become invaluable for diagnosis in those special situations where arsenicosis-simulating skin lesions pose a diagnostic challenge. There are countries where laboratory confirmation is required before a final diagnosis of arsenicosis is made. To establish an exposure, it is essential that elevated concentration of arsenic in drinking water is documented; whereas in those cases where the drinking water data is unavailable or unreliable (especially in migratory population), biological sample analysis plays an important role in the diagnosis. On the basis of arsenic metabolism data, important biomarkers of arsenic exposure are the urinary excretion of the metalloid and its concentration in hair and nail. Hematological estimation carries no value in the diagnosis because of short half-life of arsenic in blood. Estimation in water and urine Consumption of drinking water with an arsenic concentration more than the prevailing national standard for at least 6 months is essential for establishment of elevated exposure to arsenic. [4] The maximum permissible limit of arsenic in drinking water as per the recent guideline of WHO is 0.01 mg/L; so any water sample containing arsenic of concentration more than 0.01 mg/L is to be considered positive. [4] Unfortunately the countries which are the worst affected, like India and Bangladesh, are still following the previous guideline of 0.05 mg/L. This highlights the need for revision of national standard, so as to allow for more stringent diagnostic criteria as per the global standard. The concentration of total arsenic in urine has often been used as an indicator of recent arsenic exposure because urine is the main route of excretion of most arsenic species.[10],[11] It is important that the subject has not consumed any seafood for 4 days preceding urine collection for arsenic estimation.[4] Because of difficulties in collecting 24-hour urine, as well as risk of bacterial contamination during sampling; [12],[13] and the fact that arsenic excreted in urine is remarkably stable throughout a single day, [14] the first morning urine or spot urine samples are generally collected for measurement of urinary concentration of inorganic arsenic. [15] Estimation in nails and hairs Both nails and hairs provide circumstantial evidence of arsenic exposure within the preceding 9 months. [4] Analysis of nails is considered to be a good reflection of long-term exposure because nails, after rapid growth, remain isolated from other metabolic activities in the body. [16],[17] Similarly hair arsenic concentration of 1 mg/kg has been associated with levels at which health effects have been observed. [18],[19] The major concern with using nails (and also hair) as indicators of arsenicosis is the ability to account for the presence of exogenous arsenic, which may cause an overestimation of body burden. [20] A variety of techniques have been tried to wash off external arsenic, with varying degrees of success. [21] Both hair and toenail arsenic concentrations are found to increase with increasing environmental arsenic concentrations (in drinking water, in residential soil, or both) in a dose-dependant pattern. [21] In view of the fact that hair arsenic concentration is influenced by environmental contamination, appropriate measures as highlighted in [Table - 1] need to be taken during collection of hair samples. Normal arsenic values in nails appear to range from 0.02 to 0.5 mg/kg. [22],[23] A single dose of arsenic can be detected at the distal tip of the nails about 100 days after exposure.[24],[25] Toenail arsenic concentrations have been shown to be a better surrogate marker than hair arsenic concentrations because of their improved correlations with environmental concentrations as compared with hair, with low inter-individual variability. [26] Methods for the determination of arsenic in the samples (water, hair, nails, and urine) There have been several methods described for the detection of arsenic, which include colorimetric methods, atomic absorption spectrometry, inductive coupled plasma (ICP) methodology, voltammetry, radiochemical methods, x-ray spectroscopy, hyphenated techniques, etc. [27] Most of them suffer the inadequacy of being semi-quantitative or having low sensitivity. Presently atomic absorption spectrometry is considered the standard reference method (′gold standard′) because of its high specificity and sensitivity. [4] Test kits for arsenic detection: It is felt that for mass screening in field condition where sophisticated laboratory facilities are not available, a reliable test kit becomes invaluable. There are several test kits [28],[29],[30] commercially available and some are in the pipeline; [31] but till date, reliability of a single test kit has not yet been proven. Hence WHO recommends that member countries should develop policy and guidelines for selection, import, and use of these kits in consultation with their respective national control authorities. [4] Newer biomarkers of arsenic exposure Arsenicosis being a disease that needs chronic exposure (almost 10 years; range, 5-20 years) [32] before its full-blown expression, it is obvious that biomarkers that could indicate exposure would be of immense help. A study in the Guizhou Province, China, found significantly raised levels of urinary uroporphyrin-III and coproporphyrin-III (but not coproporphyrin-I) in the arsenic-exposed group as compared to controls. [33] Another study from the same area revealed metallothionein (MT), a metal-binding protein that protects against metal intoxication, was significantly lower in arsenicosis patients as compared to normal. [34]It was found that blood MT corresponds well to tissue MT levels; thus a low blood MT could predispose an individual to arsenic intoxication and thus serve as a early biomarker of toxicity. Histology as diagnostic clue Histology of keratotic papulo-nodules is not generally contributory (manifested mainly by hyperkeratosis and acanthosis) as a diagnostic marker of arsenicosis, but early detection of few dysplastic cells can point towards early premalignant change. Bowen′s disease, basal cell carcinoma (BCC), and squamous cell carcinoma (SCC) can be diagnosed by their classical histological features, and histopathological study can help in timely intervention for the treatment of keratotic lesions. On the other hand, histology of pigmented lesions has fallen out of grace due to their non-malignant potential. Control of Arsenicosis The control measures of arsenicosis revolve around the positive role of raising public awareness by information, education, and communication strategies. Arsenicosis is one of those diseases for which no effective therapy is known till date. Considering the fact that a patient once affected may not recover even after remediation, the principal focus rests on prevention of the problem. WHO has recommended 5 key approaches [4] in the management of arsenicosis: Cessation of exposure to drinking water The recent pandemic of arsenicosis is entirely due to drinking of arsenic-contaminated water; hence provision of arsenic-free water is the ultimate aim in prevention. Many new methodologies are being developed for removing the arsenic content in the water, but they have not yet passed the test of time. Hence, finding safe water sources having arsenic level below the ′maximum permissible limit′ remains the prime objective; nevertheless, methods for removal of arsenic from drinking water need to be explored. Safe water sources: A few recommendations have been put forward regarding safe water sources, which include [4],[35]
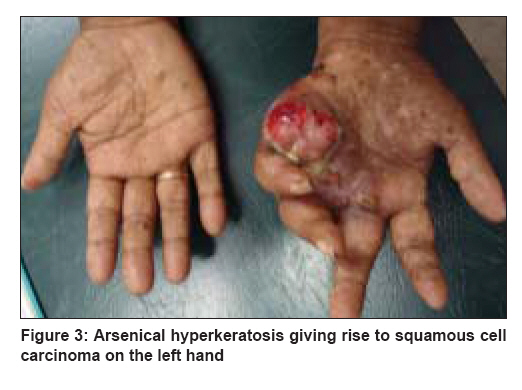
Removing arsenic from the contaminated water: In view of the large extent of arsenic contamination of ground water, repeated attempts are being made to find out an economically feasible and practically effective method for removing arsenic from drinking water. Arsenic removal plant (ARP) for big-diameter tube well and arsenic treatment unit (ATU) for hand pump-fitted tube well remain possible options to provide arsenic-free drinking water. The recent experience of the ARP is disappointing. In one of the studies on 18 ARPs, none of the ARPs could maintain arsenic in filtered water below the WHO provisional guideline value; and only 2 could meet the Indian standard value (50 µg/L) throughout. [38] Nevertheless, researches to find out an effective method are ongoing. Administration of nutritional supplement The role of nutrition in preventing the onset of symptoms of arsenicosis is highlighted in various studies . [39],[40],[41],[42],[43] People should be encouraged to take food of high calorific value from either animal or plant source, so that in spite of drinking arsenic-contaminated water, they can survive its consequences. Arsenic induces its toxic effects via generation of free radicals, [44],[45] and this brings into play the role of antioxidants in the prevention and/or treatment of arsenic toxicity. Animal study has shown that N-acetyl-L-cysteine (NAC), which modulates hepatic glutathione hydroxylase GSH level, reduces the liver injury produced by arsenic. Thus supplementation of NAC can be explored in future to reduce the arsenic-induced hepatic damage. [47] Further study on animal model with vitamin C (ascorbic acid) and vitamin E (alpha-tocopherol) has shown reduced arsenic-induced DNA damage by reducing TNF-alpha level and inhibiting the activation of caspase cascade. [48] It needs to be emphasized that antioxidants (vitamin A, alpha-tocopherol, ascorbic acid) when taken along with arsenic-free water showed significant improvement in arsenicosis.[49] Selenium (Se) in diet was shown to ameliorate the effect of arsenic toxicity. It is thought to be due to the ability of Se to complex with arsenic forming the seleno-bis (S-glutathionyl) arsinium ion, which is excreted in bile, apart from forming nontoxic insoluble selenides by complexation of Se with arsenic in tissues. Se offers additional protection by elevation of glutathione peroxidase activity, thereby reducing the oxidative stress induced by arsenic. [50] Many new agents are being tried, with optimistic results; these include spirulina, [51],[52],[53],[54] spinach extract, [55] and water hyacinth root extract. [56] Spirulina, a microscopic blue green algae, alone [51],[52],[53] or in combination with zinc, [54] is found to be effective in improving symptoms of arsenicosis. In an animal study, extracts of water hyacinth root ( Eichhornia crassipes ), which contains methionine, were found to decrease the tissue concentration of arsenic; though not as effectively as alpha-tocopherol. [56] Unfortunately, till date data on the efficacy of these antioxidants are not scrutinized through proper randomized, blinded, controlled clinical trials. Under the present circumstances, the national bodies and the recommendations of the concerned medical bodies in the respective countries decide the use of these drugs in field settings. Treatment of Arsenicosis Arsenicosis is one of those diseases for which no effective therapeutic measures are known; hence, role of preventive and supportive therapy becomes extremely important. Arsenicosis not only involves the skin but virtually all the other organ systems as described in [Table - 2]. Following measures are of prime importance in the supportive therapy: Treatment of hyperkeratinization: Thickening of the sole and palm can be treated by local application of keratolytic ointment (containing 3% salicylic acid). [57] WHO recommends the use of 5%-10% salicylic acid and 10%-20% urea-based ointment; it also highlights the need for evaluation of higher concentrations for better efficacy. [4] Apart from keratolytics, retinoids, by the virtue of their antikeratinizing effects in other disorders of keratinization, have been tried in arsenical hyperkeratosis. [58],[59] In addition to causing regression in arsenical keratosis, retinoids may offer significant promise in the chemoprevention of arsenic-related cancers by their ability to influence the expression of genes that effect cell differentiation, proliferation, and induction of apoptosis. [60] The side effects of retinoids, along with the prohibitive costs, limit their use in community-based management. Surgical intervention in mild-to-moderate keratotic papules or nodules has not been widely tried. Those lesions with sudden increase in size, cracks, and bleeding; and those of Bowen′s disease, BCC, and SCC need to be surgically excised at the earliest opportunity ( vide infra ). Treatment of GI symptoms: Dyspeptic symptoms associated with chronic arsenicosis are managed by the use of H 2 receptor blockers with/without prokinetic drugs. For noncirrhotic portal fibrosis giving rise to portal hypertension resulting in varices, sclerotherapy or banding may be needed to control the GI hemorrhage. [15] Treatment of peripheral neuropathy: Tricyclic antidepressants such as amitryptiline may have utility in relieving painful dysethesias of arsenical peripheral neuropathy. [61] Treatment of respiratory symptoms: In chronic bronchitis with or without obstruction, it is extremely important that bronchial irritation be reduced to a minimum. Smoking habits and dusty and smoke-laden atmospheres are to be avoided, and respiratory infection should be treated promptly. Bronchodilators have a limited role in interstitial lung diseases. [15] Secondary prevention of latent effects Arsenicosis is notorious for its ability to induce carcinogenesis even after stoppage of arsenic exposure. Skin is the most important visible organ where cancers like Bowen′s disease, BCC, SCC develop. These are generally late sequelae but important causes of morbidity and mortality. Urinary bladder carcinoma and pulmonary and hepatic carcinomas are also not very rare. Excision of early skin cancer [Figure - 3] and bladder cancer due to chronic arsenicosis can be curative. However, in advanced cases of these cancers and in cases of internal cancers, the treatment options are meager. This highlights the need for continuous surveillance for detection of cancer in all those exposed to arsenic-contaminated water. Counseling and education The fear of arsenicosis being a contagious disease still prevails in the minds of people, and a study on the social implication of the disease reveals a negative social impact and sharp differences of perceptions about arsenic and social issues between arsenicosis patients and unaffected people. [62] The atrocities and rejection that the patients have to face from the family and from the society are a result of ignorance about the disease. The public education programs should emphasize the adverse effects of arsenic intake (including late sequelae, like cutaneous carcinomas and systemic involvements) via drinking water; and also limited use of unsafe water for cooking; though it may be used for bathing and washing clothes. For any social program to be successful, the participation of the society is necessary, which is impossible in the absence of knowledge about the disease. In a survey, it was found that knowledge of arsenicosis rose between the 2 surveys, in 2000 and 2002, among women in Bangladesh from 42% to 64%, but awareness of consequences of arsenicosis remained limited; and only 13% knew that it could lead to death. [63] This situation needs to change, and every effort needs to be made in this regard. The public education program running at present needs to be given a serious introspection, as one of the studies found that 57% of at-risk, program-influenced survey respondents were still drinking arsenic-affected water and 54% were cooking with arsenic-affected water. [64] The experience from previous public awareness programs will help in devising more focused public education strategies that would help in the psycho-social rehabilitation of arsenic-affected people and in the prevention of the tendency of the society to ostracize these people. Role of chelation therapy A chelating agent usually has a greater affinity for the metal ion and forms ring structure with a metal which has water solubility greater than that of the offending metal and thus increases its excretion by the kidney. Chelation therapy in arsenic toxicity is thought to be a specific therapy for relief of systemic clinical manifestations and reduction of arsenic stores in the body, thereby reducing subsequent cancer risk. Chelating agents like DMSA (dimercaptosuccinic acid), DMPS (dimercaptopropane succinate), d-penicillamine have frequently been considered for treatment of chronic arsenic toxicity; however, their usefulness is yet to be established. The clinical outcome with DMSA therapy is confounding, with some studies showing good results [65],[66] while some finding it ineffective. [67],[68] It is found that combination of DMSA with long carbon chain analogues like monoisoamyl DMSA or monocyclohexyl DMSA showed a better efficacy in reducing the arsenic burden than DMSA alone. [69] On the other hand, DMPS chelation is reported to prompt increase in the excretion of arsenic in urine; [70] but its effect on long-term net excretion is cast with doubts. [71] However, a recent clinical study has reported favorable results with the use of DMPS in chronic arsenic toxicity. [72] Regarding penicillamine therapy, in spite of the initial report of improvement in arsenic-induced peripheral neuropathy, [73] further studies failed to give any favorable report. [74] Role of various levels of health care in managing arsenicosis The relentless efforts of WHO in devising a model management strategy envisage a three-tier system with primary health centers, district hospitals, and state hospitals rendering the primary, secondary, and tertiary health care services respectively; [4]
References
Copyright 2008 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv08246f3.jpg] [dv08246f2.jpg] [dv08246t3.jpg] [dv08246t2.jpg] [dv08246f1b.jpg] [dv08246t1.jpg] [dv08246f1a.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}