 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
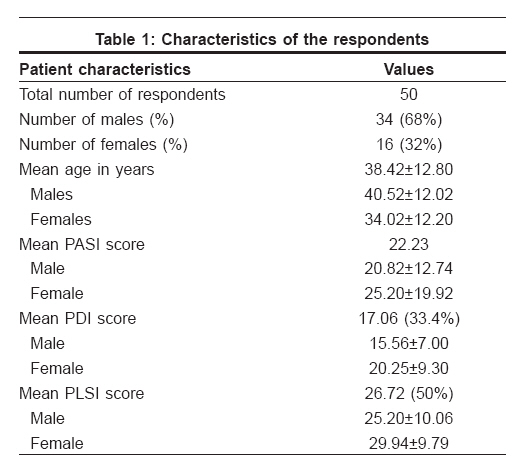
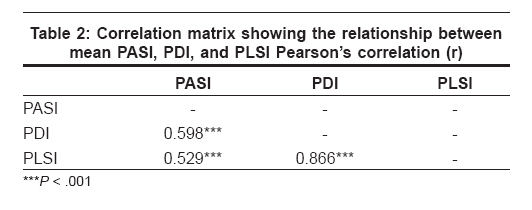
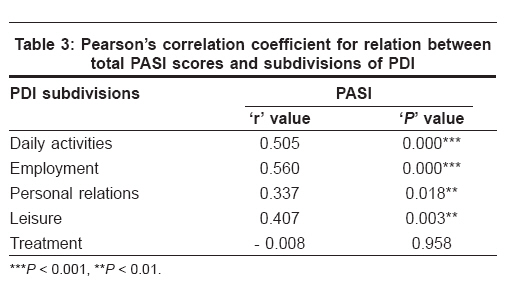
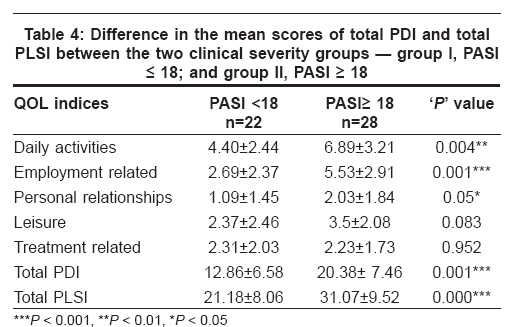
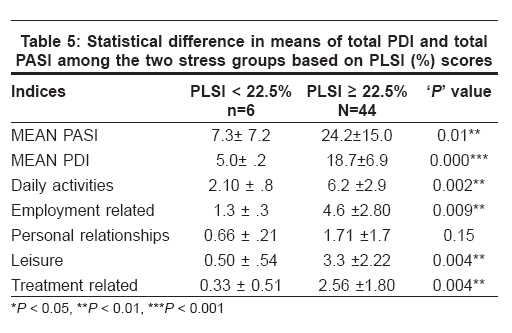
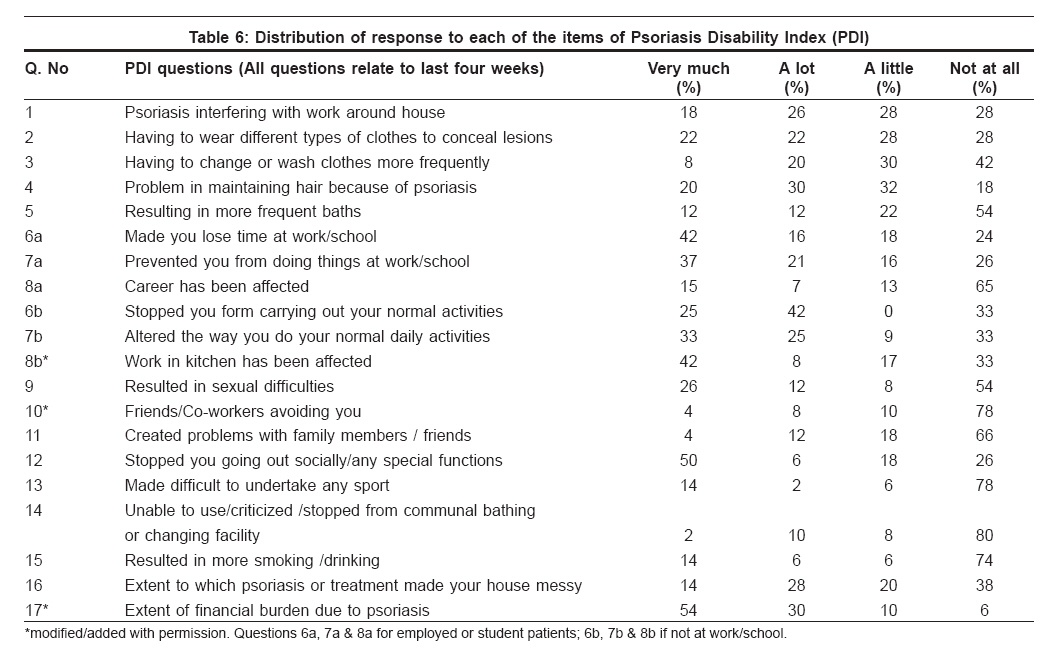
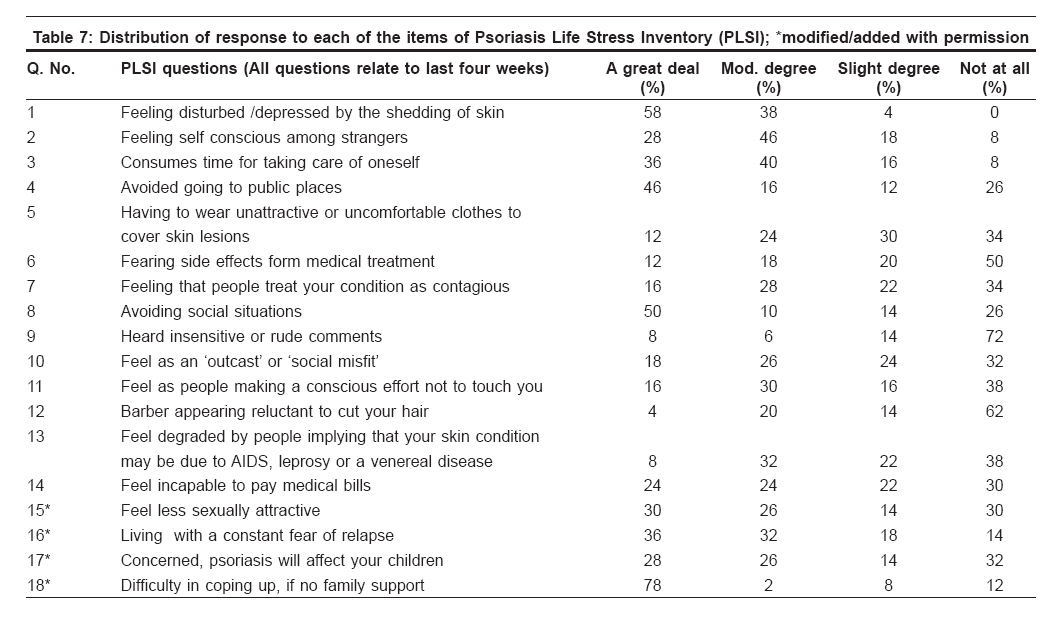
Indian Journal of Dermatology, Venereology and Leprology, Vol. 74, No. 6, November-December, 2008, pp. 600-606 Original Article Quality of life in psoriasis: A study from south India Rakhesh SV, D'Souza Mariette, Sahai Ajith Department of Dermatology and STD, Academy of Medical Sciences, Kannur, Kerala Code Number: dv08249 Abstract Background: Psoriasis can have a profound impact on a patient's quality of life. Very few Indian studies have examined this aspect of Indian patients of psoriasis.Aims: This study was conducted to assess the clinical severity, as well as physical and psychosocial disability, and stress incurred and to analyze their interrelationship in psoriasis patients aged more than 18 years. Methods: This hospital-based cross-sectional study was conducted in the Department of Dermatology, JIPMER, Pondicherry, India. Clinical severity, physical and psychosocial morbidity, and the stress incurred were measured using psoriasis area severity index (PASI), psoriasis disability index (PDI), and psoriasis life stress inventory (PLSI) respectively, the latter two of which were suitably modified and translated into the local language, viz., Tamil. Appropriate tests were conducted using SPSS for Windows (Release 7.5.1) statistical software. Results: Fifty patients (34 males, 16 females) were included in the study. The clinical PASI scores correlated significantly with the overall physical disability (PDI), individual aspects of the PDI (except the treatment-related activities), and the measurement of stress incurred (PLSI). A PASI score of more than 18 delineated a subgroup of patients with higher overall physical disability and higher stress rating. Among the physical and psychosocial factors investigated, daily activities, employment, and treatment were reported to be affected the most. Psoriasis sufferers are also most likely to feel self-conscious, be disturbed / inconvenienced by the shedding of the skin, live in a constant fear of relapse, and avoid social interactions. Conclusions: The present study provides compelling evidence that psoriasis affects the quality of life, and it highlights the importance of adopting a multidimensional assessment of psoriasis. Keywords: Multidimensional assessment, Psoriasis area severity index, Psoriasis disability index, Psoriasis life stress inventory, Quality of life Introduction Psoriasis ravages the quality of life (QOL) of afflicted individuals. It is a disease with profound impact on the psychological and social aspect of the patient, particularly because of its visibility.[1] Thus assessment by a health professional of the extent of apparent disease in terms of the clinical severity alone may not suffice, and a more holistic approach to the quality of life is mandatory.[2] Quantification of the impact of psoriasis on the QOL, along with clinical severity assessment, as has been demonstrated in various studies, could provide a measure of the clinical efficacy of the dermatological therapies; since an important concept of a favorable treatment outcome in psoriasis is the improvement in the overall psycho-social morbidity associated with the disease.[3],[4] The anguish expressed by many psoriasis patients has been explored extensively in western literature over many decades.[5] Surprisingly, very few Indian studies have looked into the psychological aspects of this chronic disfiguring disease. Thus the aims of our study were to assess the clinical severity, the physical and psychosocial disability and to analyze their interrelationship in psoriasis patients Methods The study group consisted of 50 consenting consecutive cases of psoriasis, of both sexes, aged above 18 years, and with duration of the disease of at least 3 months, attending the dermatology OPD of JIPMER, Pondicherry. The study period was from September 2000 to March 2002. The psoriatic indices assessed were psoriasis area severity index (PASI),[6] psoriasis disability index (PDI)[7] and psoriasis life stress inventory (PLSI).[8] Clinical severity The extent of clinical severity of the disease was assessed by the psoriasis area severity index (PASI).[6] Quality of life assessment Patients completed a multidimensional QOL assessment comprising the psoriasis disability index (PDI) and the psoriasis life stress inventory (PLSI). Both the questionnaires had been translated to Tamil and validated by back-translation to English by two unbiased individuals separately. Psoriasis disability The original PDI (1990 version) questionnaire was suitably modified to suit the local population.[7] The resulting score ranged from 0 to 45. The higher the score, the more the quality of life is impaired. The PDI can also be expressed as a percentage of maximum possible score of 45. As in the original questionnaire, all the questions related to events that had taken place in the preceding 4 weeks. We added two questions - "how much was the work in kitchen affected?" and "how much financial burden did you (patient) experience due to the treatment of psoriasis?" - under the subdivisions of ′work or school′ (alternative questions if not at work or school) and treatment-related questions respectively. These questions, we felt, had relevance in our cultural setting. The resulting score, thus, ranged from 0 to 51 instead of 0 to 45. For comparison with previous studies, we also expressed the total score as percentage. Psoriasis life stress We assessed the stress incurred by the patient using a modified version of the psoriasis life stress inventory (PLSI),[8] Scores on this scale ranged from 0 to 45. The scores can also be expressed as percentage scores. We found 1 question obsolete - relating to "sunbathing in the company of others" - when applied to our patients and had deleted it. Further, we added 4 questions on the basis of a preliminary interview of some of our psoriatic patients; these related to "feeling less sexually attractive," "concerned about children developing psoriasis," "fear of relapse, when disease free," "difficulty in coping with the disease if there was no family support." Thus our resulting scores ranged from 0 to 54, which were expressed as a percentage for comparison with other studies. Statistical analysis was conducted using SPSS for Windows (Release 7.5.1) statistical software. Results The study included 50 consecutive consenting patients with psoriasis attending the dermatology OPD at JIPMER, Pondicherry. The characteristics of the respondents are given in [Table - 1]. Correlation of clinical severity scores with QOL indices We observed highly significant correlation between PASI, PDI, and PLSI. The interrelationships between the 3 indices are given in [Table - 2]. The total PASI score significantly correlated with the total PDI (r = 0.598; P < 0.001) and with total PLSI (r = 0.529; P < 0.001). The percentage variability in PASI explained by a change in PDI and PLSI was 36% and 28% respectively. Total PDI significantly correlated (r = 0.866; P < 0.001) with PLSI, with percentage variability in PLSI explained by 76%. Total PDI, PASI, and PLSI were positively correlated with each other, and this relationship was found to be statistically significant. Correlation between clinical severity score and various aspects of physical disability We observed significant correlation of the PASI score with all subdivisions of PDI except treatment-related activities [Table - 3]. QOL indices in two clinical severity groups based on PASI The patients were divided into 2 groups based on their PASI scores; group I, PASI < 18; group II, PASI ? 18. The mean of the PDI and its subdivisions and the PLSI in each of the clinical severity groups were compared [Table - 4]. We found the total PDI and all its subdivisions (except questions relating to leisure and treatment) and the PLSI scores to be significantly higher in group II (PASI ? 18). Comparison of stress reactive groups based on PLSI On the basis of the PLSI scores (percentage scores), we divided our patients into 2 groups: group I - less stress reactive group, with a PLSI score of < 22.5%; group II - high stress group, with a PLSI score of ?22.5%. On comparing the 2 groups, we observed that patients classified as more reactive to stress had higher clinical severity score (PASI, P = 0.01) and higher physical disability (PDI, P < 0.001). We also observed that group II had higher mean scores in all aspects of PDI except for those related to personal relationships. The results are given in [Table - 5]. PDI and PLSI questionnaires - the response pattern The overall pattern of response, percentage of patients ticking each response in the PDI, and PLSI questionnaires are given in [Table - 6] and [Table - 7]. Discussion The psycho-social and occupational impact of psoriasis is as important as traditional physical parameters such as PASI.?[2] Although the PASI has its disadvantages, to date, it is the most adequate instrument available to evaluate clinical severity in plaque type psoriasis.[9] Both PDI and PLSI are popular tools used to assess QOL in psoriasis all over the world.[10],[8] Clinical severity and QOL indices The clinical severity measurement correlated significantly with the overall physical disability (PDI), individual aspects of the PDI (except the treatment-related activities), and the measurement of stress incurred (PLSI). Our findings were in concordance with those of other investigators like Finlay,[11] Aschroft,[12] and Gelfand,[13] who also found moderate correlation between PASI scores and PDI scores. Yang et al[14] and Fortune et al,[3] however, did not find any significant correlation between PASI scores and PDI scores. On closer examination of Fortune′s[3] study, we noted that most of his patients had low clinical severity scores (mean PASI = 8.8) as compared to our study (mean PASI = 22.23). Koo et al.[15] had demonstrated earlier that PDI is a more reliable instrument for people with severe psoriasis, who have more physical disability and limitations related to life styles. Hence the extensive clinical involvement in most of our patients causing physical disability and imposing limitations on their life styles, explains the highly significant correlation between PASI and PDI in this study. This is in contrast to Fortune′s[3] patients, who had milder disease so as not to interfere with their life styles. Recently, the psychometric properties of PDI have been analyzed, leading to the conclusion that PDI is not well targeted to measuring disease impact among patients with low levels of disability.?[16] We also observed significant correlation of the PASI scores with all subdivisions of PDI, except treatment-related activities, which failed to correlate with PASI scores. Finlay, in an earlier study,[7] had found the PASI scores to significantly correlate with all aspects of PDI. The absence of any significant correlation between the clinical severity and treatment-related activities (which included a question relating to financial burden) points towards the fact that most of our subjects were inpatients of a ′service free′ government hospital. Thus a subject with a more severe clinical disease would actually face lesser financial burden than the patient with clinically milder disease, who would have been treated as an outpatient and would have had to buy his own medicines. In our study, we observed significant correlation (r = 0.529; P < 0.001) between the overall PASI scores and the stress incurred by the patient (PLSI). Despite a thorough search of literature, we came across only one study[3] which attempted to correlate the PASI and PLSI scores. This study by Fortune[3] found no correlation between clinical severity and psoriasis life stress inventory. We assume, again, his patients with mild clinical disease probably had lower stress levels to be reflected in the overall PLSI scores. Earlier, Gupta[8] found correlation between PLSI scores and global patient self rating of clinical severity of the disease. In our study, a PASI score of more than 18 delineated a subgroup of patients with higher overall physical disability and higher stress rating. Aspects of daily activities, employment, and personal relationships were the most affected in this subgroup with higher clinical severity. Thus, a cut off point for PASI (PASI > 18), which was earlier reported [17] as an indication for starting systemic therapy, also served to delineate a subgroup of people with more or less physical disability and psychological stress. Effects of stress reactivity A PLSI score of more than 22.5% (equivalent to the standardized cut off of 10), labeled as ′high stress reactors,′ also served to identify a subgroup of patients with greater overall physical disability scores and higher clinical severity scores. Gupta,[8] and later Fortune,[3] had classified their patients on the basis of PLSI score into 2 groups: Those patients who reacted significantly to stress associated with having psoriasis (score of> 10) and those patients who were not significantly affected by psoriasis-related stress (score of ?10). For comparative purposes, we also divided our patients into 2 groups: high stress reactors (score of> 22.5%) and low stress reactors (score of ?22.5%). Our cut off value at 22.5% corresponded to their cut off value of 10, which when expressed as percentage (10/45x100) is 22.5%. We found that patients who were classified as more reactive to stress (PLSI score> 22.5%) associated with psoriasis had an earlier age of onset of the disease (P = 0.03), a higher clinical severity score (P = 0.01), and more overall physical disability (P = 0.000) in all areas of everyday life except for personal relationships. The aspects of psoriasis disability which bore significant difference in the 2 groups were daily activities (P < 0.01), employment or alternative questions (P < 0.01), leisure (P < 0.01), and treatment-related activities (P < 0.01). Fortune[3] also found that his high stress reactive patients of psoriasis perceived themselves as disabled in all areas of everyday life as assessed by PDI. Gupta[18] observed that a PLSI score of more than 10 delineated patients with greater overall psoriasis severity (P = 0.007), more cosmetically disfiguring psoriasis, greater number of flare-ups of psoriasis, and greater severity of pruritus. Analysis of pattern of response in PDI questionnaire Analysis of the PDI questionnaire on the basis of percentage of response for each aspect of disability [Figure 1] showed that questions related to daily activities, employment, and treatment-related difficulties scored the highest, and the questions related to difficulties in personal relationships and leisure activities scored the lowest. Overall, our findings bore striking resemblance to the findings in Finlay′s[19] study group with a mean score of 38.2%. In his study, the mean sub-scores of daily activities and treatment section were greater than those of the other 3 sections, the questions relating to personal relationships scoring the lowest. More than 50% of patients in his study responded with ′a lot′ or ′very much′ to 2 questions relating to clothes; questions relating to baths, sports, and home messiness. That the questions related to sports bore contrasting results with our study can be explained by the difference in the importance given to sports activities in the late adulthood between the two cultural settings. Less than 30% of patients in Finlay′s[19] study, as in our study, responded with ′a lot′ or ′very much′ to questions relating to career, problems with friends or partners, and smoking and/or alcohol. PDI has been validated against short form health survey, or SF-36 (Ware,[20] Patrick[21]); sickness impact profile, or SIP (Finlay[11]); and Salford psoriasis index, or SPI (Kirby[2]). All these investigators found overall PDI and all aspects of PDI to be affected in their psoriasis patients. Recently, Kent[22] suggested that 3 items, viz., "problems around the house/garden," "difficulties with patients′ partners or close friends," and "effect on career prospects," be dropped from the questionnaire as they were not psoriasis specific. We partially agree with his findings, especially on the latter 2 aspects as those were the questions pertaining to the least reported problems in our psoriasis patients too. Analysis of pattern of response in PLSI questionnaire Among the psycho-social measures investigated, psoriasis sufferers were found most likely to feel self conscious, be disturbed / inconvenienced by the shedding of the skin, live in a constant fear of relapse, and avoid social situations. Stressful events in which psoriasis patients were discriminated against by others were least reported [Figure 2]. The stressful events resulting from cosmetic disfigurement seem to be more prevalent in our patients. Questions relating to stressful events in which the psoriasis patients were discriminated against by others - people treating them as contagious, insensitive remarks by adults/children, barber appearing reluctant to cut hair - all were endorsed by a lower percentage of patients. The pattern of answering by our patients bore resemblance with the responses of psoriasis patients in the US (Gupta[8]). This clearly shows that the pattern of problems of psoriasis patients is universal. The stress from cosmetic disfigurement and stress from coping with physical aspects of psoriasis seem to take the highest toll as indicated by both our patients′ responses and Gupta′s[8] patients′ responses to PLSI questionnaire. To conclude, our study has highlighted the importance of adopting a multidimensional assessment of quality of life in psoriasis. Our findings may also have important implications in measurement of efficacy of dermatologic therapy and in adjunctive stress management approaches in the clinical management of psoriasis. On the basis of this study, we would recommend, as had been previously suggested,[2],[23],[24] that assessment of psoriasis severity requires a more holistic approach which encompasses both clinical and psychological measures and not merely the clinical severity assessment in isolation. Acknowledgments We are extremely grateful to Dr. Andrew Finlay and Dr. Madhulika Gupta for granting permission to use and modify the PDI and PLSI questionnaires respectively.References
Copyright 2008 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv08249t4.jpg] [dv08249t5.jpg] [dv08249t1.jpg] [dv08249t7.jpg] [dv08249t3.jpg] [dv08249t6.jpg] [dv08249t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}