 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
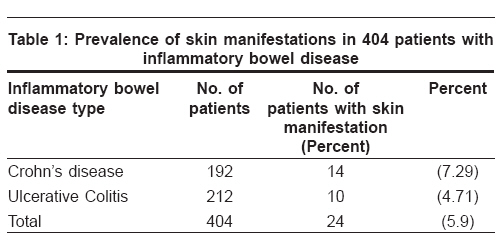
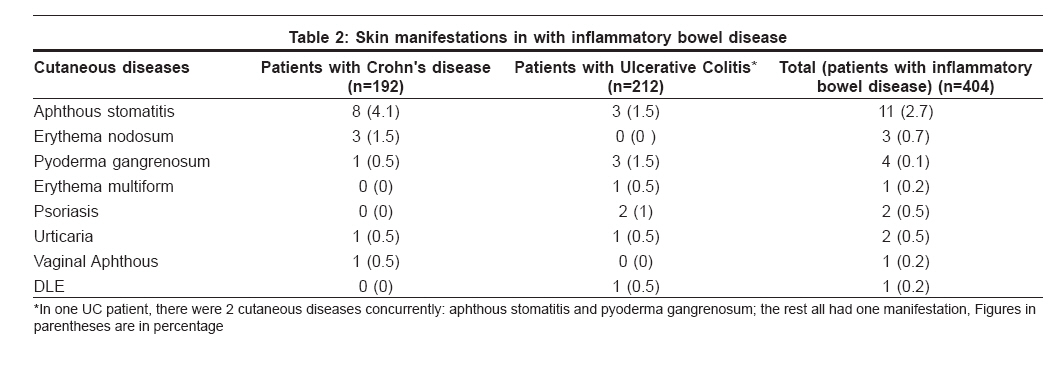
Indian Journal of Dermatology, Venereology and Leprology, Vol. 74, No. 6, November-December, 2008, pp. 607-610 Original Article Cutaneous manifestations in 404 Iranian patients with inflammatory bowel disease: A retrospective study Moravvej Hamideh, Razavi GitaMeshkat, Farshchian Mehdi, Malekzadeh Reza Skin Research Center, Shahid Beheshti Medical University, Shohada-e Tajrish Hospital, Tehran Code Number: dv08250 Abstract Background: Cutaneous manifestations of inflammatory bowel disease are relatively common, although they vary widely.Aims: The aim of this study was to determine the prevalence of cutaneous manifestations in inflammatory bowel disease according to their location, age, gender, activity, and type of underlying disease in an Iranian population during a 10-year period. Methods: The medical records of 404 inpatients with inflammatory bowel disease were extracted retrospectively to detect cutaneous manifestations. Results: In this study, the prevalence of cutaneous manifestations was 5.9%. These manifestations were higher in Crohn's disease (7.29%) than in ulcerative colitis (4.07%), and more frequent in females (52%) than in males (48%). Aphthous stomatitis was observed more frequently in Crohn's disease; however, pyoderma gangrenosum was seen more often in ulcerative colitis. Erythema nodosum was diagnosed only in female patients with Crohn's disease. Manifestations secondary to nutritional deficiency or associated conditions including psoriasis and other autoimmune disorders were less frequent. Conclusions: Aphthous stomatitis, pyoderma gangrenosum, and erythema nodosum were the most common skin disorders related to inflammatory bowel disease (IBD), which mainly occurred in women. Keywords: Aphthous ulceration, Crohn′s disease, Erythema nodosum, Pyoderma gangrenosum, Ulcerative colitis Introduction Inflammatory bowel disease (IBD) comprises 2 major disorders: ulcerative colitis (UC) and Crohn′s disease (CD). The pathogenesis of these inflammatory diseases remains poorly understood to this date. These disorders have distinct pathologic and clinical characteristics, including several extra-intestinal manifestations in various organ systems. The frequency of these manifestations varies from 6% to 46% in different countries. [1],[2],[3],[4] Cutaneous manifestations are well-recognized complications of Crohn′s disease and ulcerative colitis. The incidence of these manifestations varies widely; but at the time of diagnosis, the mean incidence is around 10%. However, a great variety of skin lesions may develop during the course of the disease. These manifestations fall into several categories: direct involvement contiguous with the bowel, reactive skin eruptions, malabsorption, skin changes secondary to cutaneous drug reactions, and other associated dermatoses. [5] Direct cutaneous involvement contiguous with the bowel consists of fissures, fistulae, and perineal abscesses, which are seen more commonly in Crohn′s disease. [6] Moreover, oral mucosa and lips may be involved in Crohn′s disease.[7] Occasionally trunks and limbs may also be involved with granulomatous lesions, namely, metastatic Crohn′s disease.[8] Reactive skin eruptions include a variety of cutaneous manifestations such as erythema nodosum, [5],[9] aphthous ulcerations, [10] neutrophilic dermatoses [10],[11] (i.e., pyoderma gangrenosum and pyostomatitis vegetans, acute febrile neutrophilic dermatosis and other vesicopustular eruptions), and erythema multiforme. [12] These skin conditions can be related to the inflammatory pathogenesis of the disease or may be at times be side effects of the treatments used in these patients or may occur in the setting of other medical problem. [5],[9],[10],[11],[12] Among these reactive eruptions, aphthous ulceration, some forms of neutrophilic dermatosis (e.g., acute febrile neutrophilic dermatoses), pyoderma gangrenosum, and pyodermatitis-pyostomatitis vegetans are more commonly observed in the setting of ulcerative colitis. [9],[10],[11] Inflammatory bowel diseases, in particular ulcerative colitis, may be also accompanied by vasculitis and intravascular coagulation disorders. [7] Furthermore, other cutaneous disorders like linear IgA disease [13] and acne (synovitis-acne-pustulosis-hyperostosis-osteitis [SAPHO] syndrome) [14] are associated with inflammatory bowel disease. . The prevalence of these various extra-intestinal manifestations shows vast differences according to the geographical area. Therefore, we undertook this study to define the prevalence of mucocutaneous manifestations in inflammatory bowel diseases in a 10-year follow-up study in Iranian IBD patients in order to better understand IBD′s characteristics in our region. Methods In this case series, medical records of 404 inpatients with inflammatory bowel disease (IBD) - Crohn′s disease and ulcerative colitis - between the years 1995 and 2005 at the Department of Gastroenterology and Hepatology of Dr. Shariaty Hospital, Tehran Medical University, were screened for extra-intestinal symptoms with special regard to cutaneous manifestations. All patients underwent a detailed whole body examination under the supervision of the senior gastroenterologist and dermatologist periodically at each visit. Diagnosis of IBD had been confirmed by clinical, endoscopic, radiological, and histological criteria as described by Lennard-Jones. [15] Mucocutaneous manifestations were investigated by a dermatologist and a dermatopathologist clinically and histologically respectively. Aphthous ulceration, erythema nodosum, pyoderma gangrenosum, pyodermatitis-pyostomatitis vegetans, erythema multiforme, vasculitis, fissures, fistulae, perineal abscesses, other granulomatous lesions occurring at sites not contiguous with the bowel such as trunk and limbs (namely, metastatic Crohn′s disease), acne fulminans, and other mucocutaneous disorders were evaluated during these visits. A questionnaire was designed to gather initial data regarding the demographic and clinical features, extra-intestinal manifestations, the extension of disease, presence of inflammatory bowel disease in relatives, surgical interventions, treatments; and later to evaluate each follow-up visit performed by the physicians in 212 ulcerative colitis patients and 192 Crohn′s disease patients. These data were gathered by face-to-face interview and were also retrieved from the medical files of the patients. As for the extra-intestinal manifestations, we examined their nature and also looked to find out if they appeared before, concurrent with, or after the expression of the intestinal manifestations of IBD. Results During the years 1995-2005, 404 patients were identified to have IBD. Among these, 212 (52.5%) were diagnosed as having ulcerative colitis, and 192 (47.5%) were diagnosed to have Crohn′s disease ( P value < .001). The age at presentation varied between 8 and 81 years. The mean age of IBD patients at the time of diagnosis was 31.2 years. The mean ages of patients harboring Crohn′s disease and ulcerative colitis were 30.62 and 31.73 years respectively. The minimum age of presentation was 8 years, in an ulcerative colitis patient; and the maximum age of presentation was 81 years, in a Crohn′s disease patient. Ulcerative colitis patients consisted of 120 (56.6%) females and 92 (43.4 %) males, and Crohn′s disease patients included 96 (50%) females and 96 (50%) males. All in all, our patient population was formed by 216 females and 188 males. We analyzed the data regarding the mucocutaneous manifestations in our patients and obtained the following results. The prevalence of cutaneous manifestations in our IBD patients was 5.9% (24/404), which consisted of 14 cases in Crohn′s disease patients (14 out of 192 patients) and 10 cases in ulcerative colitis patients (10 out of 212 patients) [Table - 1]. Of the 192 Crohn′s disease patients, 8 (4.2%) had aphthous stomatitis, 3 (1.6%) had erythema nodosum, 1 (0.5%) had pyoderma gangrenosum, 1 (0.5%) had urticaria, and 1 (0.5%) had vaginal aphthous ulcers. Among the 212 ulcerative colitis patients, 3 (1.4%) had aphthous stomatitis; 3 (1.4%) had pyoderma gangrenosum; 2 (0.9%) had psoriasis developed within 2 years after onset of IBD, among whom 1 only had toe nail psoriasis; 1 (0.5%) had urticaria; 1 (0.5%) had erythema multiforme; 1 (0.5%) had discoid lupus erythematosus. In 1 of our patients (female patient with ulcerative colitis and age of 50 years), we observed 2 cutaneous manifestations concurrently (aphthous stomatitis and pyoderma gangrenosum). Rest of the patients demonstrated only 1 skin problem [Table - 2]. However, we did not identify any patients with rosacea, acrodermatitis entropathica, metastatic cutaneous Crohn′s disease, fissures, fistulae, perineal abscess, or with involvement of lips and oral mucosa (cobblestoning). According to our findings, aphthous stomatitis was the most common cutaneous manifestation, present in 11 (41.6%) out of 24 of all IBD cases which showed skin lesions; and the majority of these patients were those with Crohn′s disease (8 out of 11 patients). Furthermore, pyoderma gangrenosum took the second place, including 4 (16.6%) out of 24 patients of all IBD patients with cutaneous manifestations; and it was more commonly observed in ulcerative colitis patients. Erythema nodosum was diagnosed in 3 (12.5%) out of 24 patients, all of whom were females with Crohn′s disease. In general, the prevalence of cutaneous manifestations was higher in Crohn′s disease (7.29%) in comparison with ulcerative colitis (4.71%). Discussion Inflammatory bowel diseases are occasionally accompanied by cutaneous manifestations. These cutaneous manifestations can be either contiguous with the bowel or a reactive cutaneous eruption or may even occur due to drug reactions or other etiologies not well understood. Moreover, these cutaneous lesions can occur prior to, concurrent with, or after the manifestation of the gastrointestinal problems.[1],[2],[3],[4] Various forms of skin lesions have been described in association with inflammatory bowel diseases, including aphthous stomatitis, pyoderma gangrenosum, erythema nodosum, erythema multiforme, psoriasis [5],[9],[10],[11],[12] (mostly described in association with Crohn′s disease), [16] fissures, fistulae, perineal abscesses, [6] granulomatous cheilitis, [8] granulomatous rosacea, [17] metastatic cutaneous Crohn′s disease, [8] and acrodermatitis enteropathica. [18] Also therapeutic regimens used in these disorders may result in problems such as acne, striae, moon facies, and erythema. The prevalence of these cutaneous disorders in IBD patients varies considerably depending on the geographical region. Therefore, it is of great importance to know the characteristics of these manifestations in different regions. Our study, even though a retrospective one, was very thorough; because during the long term of follow-up, all patients were examined and interviewed at each visit by a gastroenterologist and a dermatologist with the supervision of a dermatopathologist. Our results show some distinctions from those of the studies performed previously in other areas. For instance, we tracked aphthous stomatitis more commonly in Crohn′s disease patients, which is in contrast to the findings of other studies where this entity was more common in ulcerative colitis. [10] As for erythema nodosum, some studies support the theory that it is the most frequent cutaneous manifestation of inflammatory bowel diseases, occurring mostly in women with Crohn′s disease. [4],[18],[19] In our patient population, even though we observed erythema nodosum only in women with Crohn′s disease, its prevalence was only 0.7%. Pyoderma gangrenosum′s prevalence has been estimated to be about 27.3% in patients with inflammatory bowel disease. [19] However, in our patient population, this prevalence was 0.1% (1.5% in ulcerative colitis patients and 0.5% in Crohn′s disease patients). Incidence of pyoderma gangrenosum in different entities of inflammatory bowel disease has been a matter of controversy in different studies. [19],[20] Some point to an equal incidence in Crohn′s disease and ulcerative colitis, [19] but some state a higher incidence in Crohn′s disease. [20] In our patient population, skin lesions of pyoderma gangrenosum were mostly located below the knees, which is in agreement with other studies. [21] In inflammatory bowel disease patients, aphthous stomatitis, pyoderma gangrenosum, and erythema nodosum were the most common skin disorders observed, which mainly occurred in women. Other skin disorders such as psoriasis, urticaria, erythema multiforme, vaginal aphthous ulcers, and discoid lupus erythematosus were infrequently detected. Other cutaneous manifestations were not observed in this patient population. References
Copyright 2008 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv08250t1.jpg] [dv08250t2.jpg] |
| |||||||||

{kind=link}
{kind=link}