 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
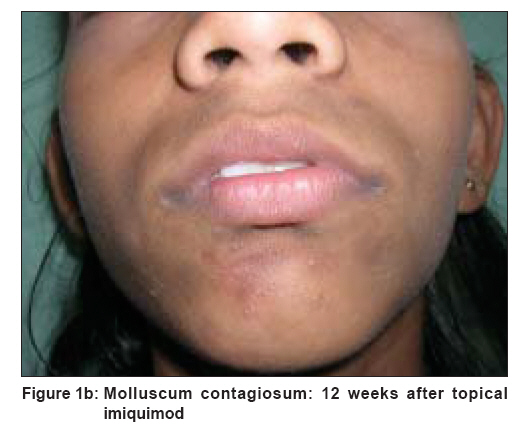
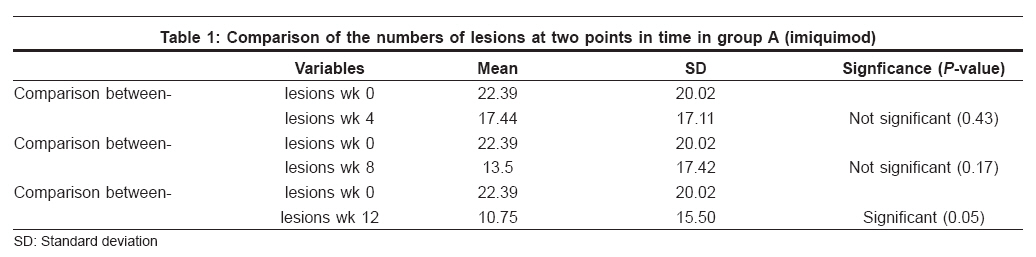
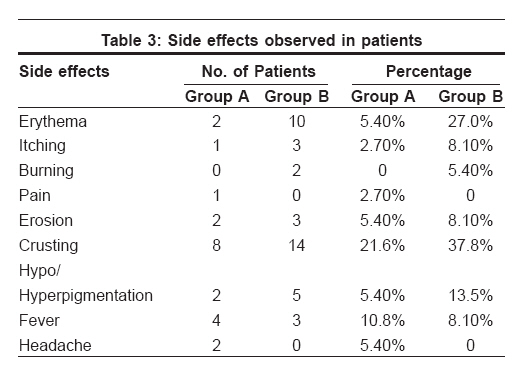
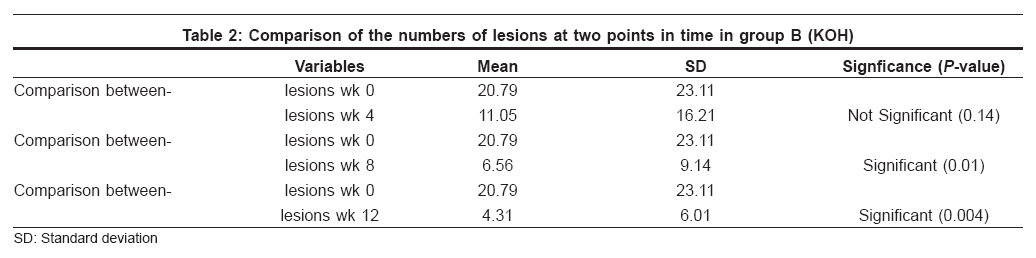
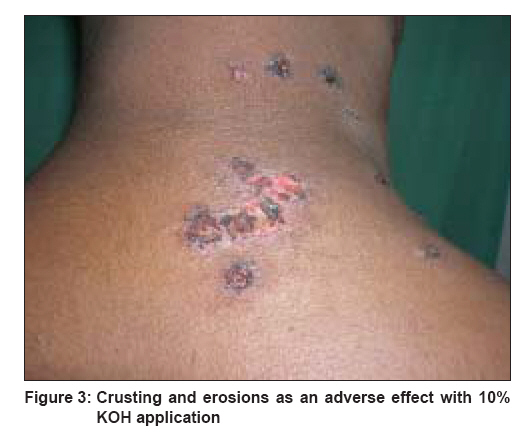
Indian Journal of Dermatology, Venereology and Leprology, Vol. 74, No. 6, November-December, 2008, pp. 614-618 Original Article An open, nonrandomized, comparative study of imiquimod 5% cream versus 10% potassium hydroxide solution in the treatment of molluscum contagiosum Metkar Amol, Pande Sushil, Khopkar Uday Department of Dermatology, Seth GS Medical College and KEM Hospital, Mumbai Code Number: dv08252 Abstract Background: There are numerous therapeutic modalities available for treatment of molluscum contagiosum. However, the ablative modalities are painful and not suitable for children.Aim: We aimed to evaluate and compare the safety and efficacy of 2 of the painless modalities, viz., 5% imiquimod cream and 10% potassium hydroxide (KOH) solution, in the treatment of molluscum contagiosum. Methods: Out of a total of 40 patients of molluscum contagiosum in the study, 18 patients in the imiquimod group and 19 patients in the KOH group completed the study. The given medication was applied by the patient or a parent to mollusca at night, 3 days per week. Imiquimod was continued till clinical cure; and 10% KOH, till lesions showed signs of inflammation. Assessments of response and side effects were performed at the end of week 4, week 8, and week 12. Significance was tested by Student's t test and Mann-Whitney test. Results: The mean lesion count decreased from 22.39 to 10.75 with imiquimod and from 20.79 to 4.31 with KOH at the end of 12 weeks. We found complete clearance of lesions in 8 (44%) patients with imiquimod and in 8 (42.1%) patients with 10% KOH. Minor side effects were seen in 15 (78.9%) patients on KOH and 10 (55.5%) patients on imiquimod. Conclusions: The results of this study suggest that both 5% imiquimod cream and 10% KOH solution are equally effective in molluscum contagiosum though KOH has a faster onset of action. However, KOH solution is associated with a higher incidence of side effects. Keywords: Imiquimod, Molluscum contagiosum, Potassium hydroxide Introduction Molluscum contagiosum is one of the commonest cutaneous viral infections seen in children and adults. The infection poses vexing treatment problems though various treatment options are available, like curettage, cryosurgery, trichloroacetic acid, cantharidin, etc. All current treatment modalities are associated with substantial pain, tissue destruction, and frequent recurrence. [1],[2] However, these procedures are not well tolerated by children owing to pain and fear. [3] These procedures are also not feasible for widespread lesions although some dermato-surgeons have performed them under general anesthesia.[4] KOH is known to penetrate deeply and destroy the skin because it dissolves keratin. [5] Ten percent potassium hydroxide (KOH) solution has been prescribed for mollusca to be applied at home and has the added advantage of being relatively painless. Recently, imiquimod, a topical immune response modifier, has been successfully used in the treatment of external anogenital warts. [6],[7],[8] Mechanism of action is the induction of cell-mediated immunity, which helps in the regression of mollusca - similar to that observed in viral warts. [9],[10] The principal antiviral cytokine, interferon-g (in addition to other inflammatory cytokines), is induced by imiquimod cream. The aim of this study was to evaluate and compare the efficacy, side effects of imiquimod 5% cream and 10% potassium hydroxide solution in molluscum contagiosum. Methods This is an open, longitudinal, nonrandomized study carried out in a tertiary care center after obtaining permission from the institutional ethics committee. Forty patients aged between 1 and 40 years, attending the dermatology outpatient department, presenting with clinical features of molluscum contagiosum were included in the study after obtaining an informed consent. For the patients under 18 years of age, consent was obtained from their parents or guardians; there being no minors above 12 years of age. A detailed history was taken, and patients underwent thorough general, cutaneous, and systemic examination. Information regarding age, sex, number of lesions, duration of illness, site of involvement, family history, history of atopy, previous treatment taken was noted. Pregnancy was ruled out by doing urinary pregnancy test in women of reproductive age. ELISA test for immunodeficiency virus (HIV) antibody was not done as most of our patients were from the pediatric age group. The inclusion criterion was the presence of minimum 3 lesions in patients who were willing to follow up. Patients with more than 100 lesions, eyelid involvement, secondary infection, and history of hypersensitivity to imiquimod were excluded. Pregnant females were also excluded from the study. Patients were divided into 2 groups, each of 20 patients. Patients were randomly allocated into 2 groups by the method of ′alternation.′ Group A was treated with imiquimod 5% cream, and group B was treated with 10% potassium hydroxide (KOH) solution. Patients or their parents were asked to apply medication at night and to wash it off in the morning. KOH (10%) solution was applied with a cotton swab, whereas imiquimod (5%) cream was applied directly on the lesion 3 times per week for 12 weeks. Patients or parents were advised to apply KOH (10%) solution on the lesional skin only and to avoid spillage onto normal skin. If accidental spillage occurred, they were advised to wash the skin with water immediately. Application of KOH (10%) solution was continued till the lesions showed signs of inflammation or superficial ulceration. Imiquimod (5%) cream was applied till the lesions subsided completely. Imiquimod (Imiquad ® , Glenmark Pharmaceuticals TM Ltd.,) was given in 0.25 g sachets. Each sachet contained sufficient cream to cover area of up to 20 cm 2 . A thin layer was applied to the lesion and rubbed in until no longer visible. Patients or parents were advised to wash hands before and after application of the drug. At the initial visit and then at 4, 8, and 12 weeks of treatment, the molluscum lesions were counted, temperature was recorded, and photographic assessment was done. Patients and parents were asked to report local (erythema, itching, burning, pain, erosion, crusting) and systemic (fever, influenza-like illness, diarrhea, headache, myalgia) side effects. If the lesions cleared early, the treatment period could be less than 12 weeks. Significance was tested by Student t test, and a P value of less than 0.05 was considered to be statistically significant. Efficacies of these 2 treatments were compared by Mann-Whitney test. Results Out of the 40 patients, 3 patients were noncompliant and did not follow up; hence 37 patients were available for efficacy analysis. The age of the patients ranged from 2 to 32 years. Most (62.5%) of the cases were in the age group of 1 to 12 years. In this study, 21 cases were males and 19 were females. Maximum numbers of patients were having molluscum contagiosum since less than 3 months. The minimum duration of infection was 15 days, and maximum duration was 1 year. History of similar complaints in the family was noted in 8 cases. History of atopy was recorded in 4 cases. The number of lesions varied from 4 to 96 (mean 22.2). Out of the 40 patients, 26 (65%) had lesions on the face while 10 (25%) patients had trunk involvement. Only 4 patients had lesions on the genitals. We found complete clearance of lesions in 8 (44%) out of 18 patients with imiquimod, of which 5 patients were cleared of lesions by 4 weeks of treatment; and the other 3, by 8 weeks of treatment. We observed total clearance of lesions in 8 (42.1%) out of 19 patients with 10% KOH. Out of these 8 patients, 6 patients were cleared of lesions by 4 weeks of treatment; and the other 2 patients, by 8 weeks of treatment. Response to treatment was seen irrespective of duration of disease and site of involvement. The mean lesion count (mean number of mollusca) decreased from 22.39±20.02SD to 10.75±15.50SD at the end of 12 weeks in patients treated with imiquimod [Figure 1a] and [Figure 1b]. The numbers of lesions at any 2 junctures during follow up were compared by paired t test. The comparison between the number of lesions at baseline (week 0) and the number of lesions at week 12 was found to be statistically significant ( P value-0.05) in group A patients. [Table - 1]. The mean lesion count decreased from 20.79±23.11SD to 4.31±6SD at the end of 12 weeks with 10% KOH solution. This reduction in number of lesions at the end of 12 weeks was statistically significant ( P value- 0.004). Similarly at the end of 8 weeks, reduction in mean lesion count (from 20.79±23.11SD to 6.56±9.14SD) was also statistically significant [Table - 2], [Figure 2a] and [Figure 2b]. However, reduction of mean lesion count at the end of 4 weeks was not found to be statistically significant [Table - 2]. The numbers of lesions at various junctures were compared between group A and group B by nonparametric tests. The differences between the numbers of lesions at various points in time between the 2 groups were not statistically significant ( P value> .05, Mann-Whitney test). Fifteen (78.9%) out of 19 patients on KOH developed side effects, whereas 10 (55.5%) out of 18 patients on imiquimod developed side effects. The commonest side effects observed were erythema and crusting [Figure - 3] in both the groups. Most of the patients complained of mild stinging sensation after KOH application, which lasted for 1 to 2 minutes. Development of hypopigmentation or hyperpigmentation was seen after treatment with KOH, which in most cases resolved spontaneously. One patient developed secondary bacterial infection, which was confirmed on Gram′s stain. He was treated with systemic antibiotic and analgesic. Systemic side effects of imiquimod, like myalgia, diarrhea, and influenza-like symptoms, were not seen. No significant difference in side effects was seen in individuals with atopy. No patient discontinued treatment because of side effects [Table - 3]. Discussion We found both 10% KOH solution and 5% imiquimod cream equally effective in the treatment of molluscum contagiosum. There was no significant difference in their efficacies. However, faster clearance of lesions was achieved by 10% KOH solution as compared to imiquimod 5% cream. Relatively long time to show resolution (after 12 weeks) and inflammatory response before clearing of lesions suggests cell-mediated immune response with imiquimod. [9],[10] Syed et al. [11] treated males having molluscum contagiosum with an analog of imiquimod 1% in cream. The medication was self administered by the patients on their lesions at home, 3 times daily for 5 consecutive days per week for 4 weeks. The frequent application of medication in this study may be due to the lower concentration of imiquimod. Barba et al. [12] treated 13 children with topical imiquimod 5% cream every night for 4 weeks. All the above studies indicate that the concentration of imiquimod and frequency of application require further evaluation. Hengge et al. [13] noted improvement in 12 out of 15 patients with 5% imiquimod. They found that 8 (53%) patients with mollusca achieved total clearance, and 4 (27%) patients showed> 50% reduction in molluscum size. The percentage of patients who were cleared of all lesions was comparable to that in our study. Side effects were more common with 10% KOH solution. Romiti et al. [14] also reported a study in which patients were instructed to apply 5% KOH solution twice a day. This was done in an attempt to reduce the side effects observed with higher concentration. [14] They found 5% KOH as effective and less irritating when compared to 10% KOH. [14] Both 10% KOH solution and imiquimod 5% cream have advantages over other treatment options viz. being less traumatic, less painful, and suited to self administration. These characteristic make them particularly helpful in the treatment of children with molluscum contagiosum. Considering the low cost and faster clearance of lesions with KOH solution, it appears to be a better option in the treatment of molluscum contagiosum. The only disadvantage of higher irritancy potential as compared to imiquimod can be taken care of by educating the parents about the correct method of application, identification of early signs of irritation and measures for prevention/early treatment of irritation. Thus this side effect is preventable, promptly identifiable and treatable with some pro-active efforts on the part of the dermatologist. In conclusion, while imiquimod cream provides a minimally irritating and more standardized form of non-invasive therapy for molluscum contagiosum, in a developing country like ours, KOH solution offers an affordable and equally efficacious and even faster acting option, albeit with a higher chance of irritant dermatitis. Acknowledgment We thank Gracewell ® division of Glenmark Pharmaceuticals Ltd. for providing imiquimod cream for this investigator initiated study.References
Copyright 2008 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv08252f3.jpg] [dv08252f1b.jpg] [dv08252t2.jpg] [dv08252t1.jpg] [dv08252f2b.jpg] [dv08252f1a.jpg] [dv08252t3.jpg] [dv08252f2a.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}