 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
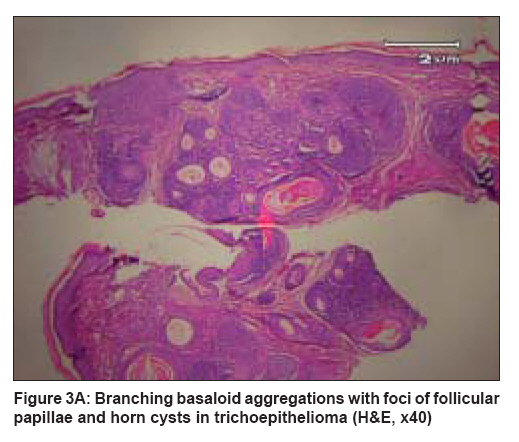
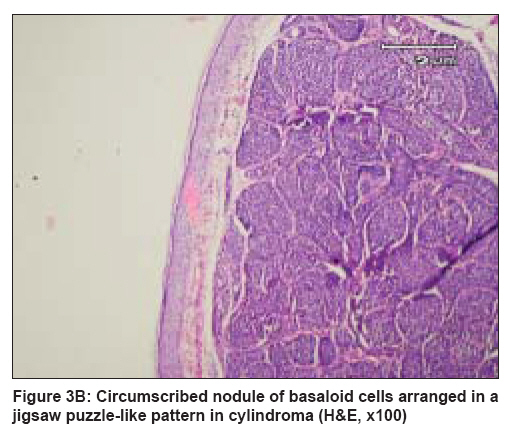
Indian Journal of Dermatology, Venereology and Leprology, Vol. 74, No. 6, November-December, 2008, pp. 632-634 Case Report Brooke-Spiegler syndrome Layegh Pouran, Sharifi-Sistani Nourieh, Abadian Mohammad, Moghiman Toktam Qaem Hospital, Mashad University of Medical Sciences, Mashad Code Number: dv08257 Abstract The Brooke-Spiegler syndrome (BSS) is an uncommon autosomal dominant disorder characterized by a high affinity to form multiple adnexal neoplasia (skin appendage tumors), especially trichoepitheliomas and cylindromas, and occasionally spiradenomas, which usually appear in the second or third decade of life. To date, only a few cases with this syndrome have been reported. This case report describes a 26-year-old woman who presented to the dermatology department of Qaem Hospital with tumoral lesions on her scalp, face, and forearm. Her father and younger brother were also affected. On examination, several round-to-oval skin-colored papules with a smooth pearly surface measuring 2 to 6 mm in diameter were seen on the mid-face, particularly in the nasolabial folds, the upper lip. Tumors and nodules seen on the scalp were pinkish red, dome-shaped, and to some extent, pedunculated with surface telangiectasia and induration. Histopathology of the facial papules showed trichoepithelioma while that of a scalp nodule showed cylindroma.Keywords: Brook-Spiegler syndrome, Cylindroma, Trichoepithelioma Introduction The Brooke-Spiegler syndrome (BSS) is an uncommon autosomal dominant disorder characterized by a high affinity to form multiple trichoepitheliomas and cylindromas, and occasionally spiradenomas. To date, only a few cases with this syndrome have been reported. We report here a patient with this rare conditionCase Report A 26-year-old female patient was presented with cutaneous lesions on her scalp and face. These lesions first appeared when she was 14 years old, primarily on her scalp and later developed on the face and had gradually increased in size and number over the years. Her father and 13-year-old brother also had similar lesions on their faces. On examination, a group of round-to-oval skin-colored papules with a smooth pearly surface measuring 2 to 6 mm in diameter was seen on the mid-face, particularly in the nasolabial folds, the upper lip, and less commonly on the forehead and the periocular areas [Figure - 1]. In addition to this, a variety of tumoral and nodular lesions was also seen on the scalp. The tumors of the scalp were pinkish red, dome-shaped, and to some extent, pedunculated with surface telangiectasia and induration. They measured 0.5 to 1.5 cm in diameter; the larger lesions were hairless, and the smaller ones had less hair than normal [Figure - 2]. There was also a subcutaneous firm nodule with a size of 0.5x0.5 cm on the patient´s right forearm. Her general condition was good. She had no known underlying disease and no previous history of taking any kind of medications. The histopathology of the scalp nodule revealed a dermal lesion with well-defined borders composed of islands of basaloid cells arranged in a jigsaw puzzle-like pattern and separated by hyaline basement membrane material. Two populations of basaloid cells (with a large nucleus centrally and smaller nuclei in a palisading pattern on the periphery) were observed, suggestive of cylindroma [Figure 3A]. In the facial papules, basaloid inclusions with immature (basic) follicular papillae and horn cysts were seen, which were surrounded by fibrous stroma and were typical of trichoepithelioma [Figure 3B]. The patient′s forearm nodule was composed of sheets of small dark-staining basaloid cells peripherally and larger cells with paler nuclei centrally, consistent with spiradenoma. According to clinical features and histopathologic findings, a diagnosis of Brooke-Spiegler syndrome (BSS) was made. In this patient, a number of large trichoepitheliomal lesions of the face and cylindromas of the scalp were finally excised; and because of the numerous lesions distributed throughout the face, she was subjected to continued treatment with carbon dioxide laser. Discussion We have presented a case with BSS. This syndrome has an autosomal dominant mode of inheritance and tends to form numerous adnexal tumors, in particular trichoepithelioma, cylindroma, and occasionally spiradenoma, especially in the second or third decade of life. [1],[2],[3],[4] To date, the cell-type specific origin of BSS is a topic of ongoing debate. For cylindroma and spiradenoma, both the apocrine and eccrine origins have been suggested, but the origin of follicular trichoepithelioma is not yet confirmed. [5] Some individuals may present with isolated trichoepithelioma or cylindroma, whereas others can have a combination of them in one tumor, as described by Honag Ly et al, [6] which suggests a common embryonic relationship between the follicles and the apocrine glands. Thus BSS represents a genetical disorder which affects the regulation of the folliculo-sebaceous apocrine unit. Further evidence for this hypothesis is provided by reports of other follicular tumors, such as BCC, follicular cyst, and nevus sebaceous, associated with this syndrome. [7],[8],[9] These findings indicate that a mutation in the genes that regulate the stem cell proliferation and differentiation can cause a defect in the differentiation of the folliculo-sebaceous apocrine unit, which gives rise to different combinations of adnexal skin tumors. [10] Genetical studies have demonstrated that mutations in the CYLD 1 gene are responsible in this disease. [11] The penetrance of the gene has been estimated to be between 60% and 100%. [6] The disease also demonstrated variable clinical and histopathological features among the affected members of a single family, in which older members tend to have larger lesions that are also greater in number as compared to the younger members. [12],[13] This condition was obvious in our patient′s family, where the younger brother (13 years old) had numerous trichoepithelioma lesions on his face. Another fact which should be importantly taken into consideration in this case is that such patients are at risk for developing BCC from trichoepithelioma, and they should be followed up and clearly informed to visit the clinic if the lesions increase in number or become ulcerated. The differed modes of treatment which have been suggested for the adnexal tumors in BSS patients include excision of the tumor, dermabrasion, electrodessication, cryotherapy, and radiotherapy using argon and Co2 lasers. In another study, it was observed that treatment with erbium-YAG laser causes less scars and fewer recurrences. It has been proven that the administration of aspirin and its derivatives can result in the rapid formation of new lesions. [14] References
Copyright 2008 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv08257f2.jpg] [dv08257f1.jpg] [dv08257f3b.jpg] [dv08257f3a.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}