 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
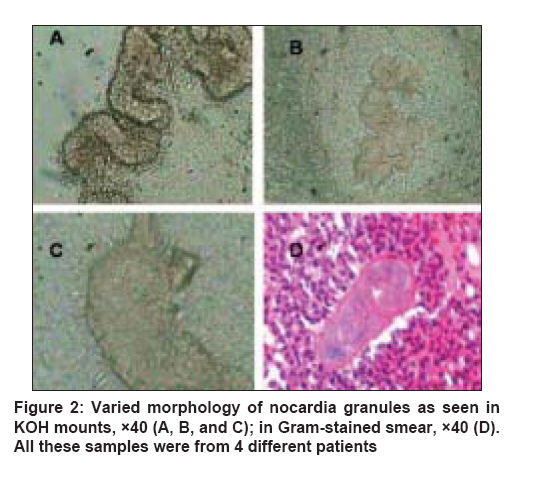
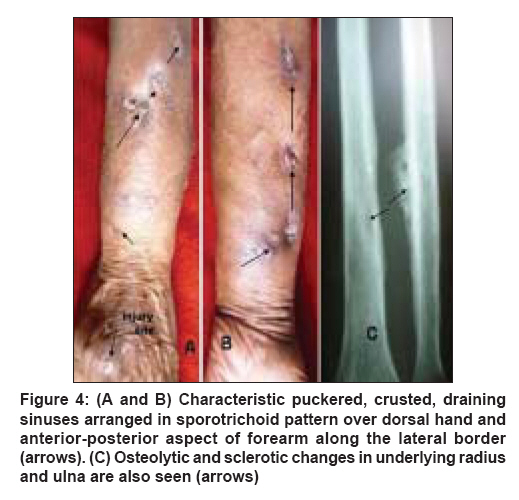
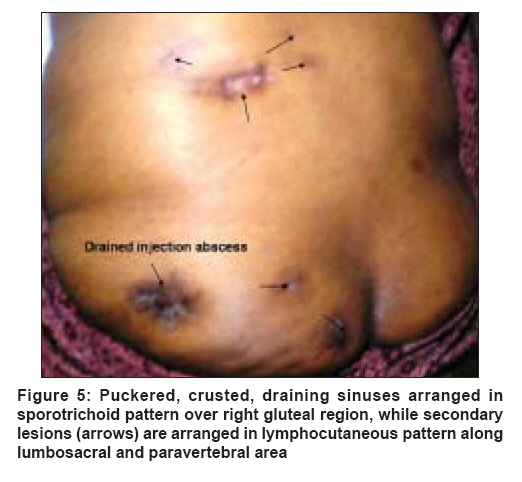
Indian Journal of Dermatology, Venereology and Leprology, Vol. 74, No. 6, November-December, 2008, pp. 635-640 Case Report Nocardial mycetoma: Diverse clinical presentations Sharma NandLal, Mahajan VikramK, Agarwal Santwana, Katoch VishwaMohan, Das Ram, Kashyap Meera, Gupta Poonam, Verma GhanshyamK Department of Dermatology, Venereology and Leprosy, Indira Gandhi Medical College, Shimla Code Number: dv08258 Abstract Nocardia spp are gram-positive, aerobic, acid-fast bacteria which exist as saprophytes in nature. Invasive disseminated infections are particularly common in immunocompromised or debilitated hosts. Superficial infections with Nocardia spp occur as a result of local trauma and contamination of the wound. Clinically, it presents as acute infection (abscesses or cellulitis), mycetoma, or sporotrichoid infection. Differential diagnosis includes eumycetoma, chromomycosis, blastomycosis, coccidioidomycosis, sporotrichosis, tuberculosis, botryomycosis, syphilis, yaws, and neoplasia. Its diagnosis is confirmed by demonstrating the causative organism in exudates (as granules), tissue specimens, or cultures. Early diagnosis will obviate need for drastic surgical measures as early institution of chemotherapy is effective in most patients. However, its diagnosis is often delayed due to diverse clinical presentations and for want of clinical suspicion, particularly in non-endemic areas. This paper presents 4 clinical forms of this not so uncommon disease, emphasizing the importance of high index of clinical suspicion, especially in non-endemic regions; and the significance of repeated examination of exudates for Nocardia granules for an early diagnosis.Keywords: Himachal Pradesh, Maduromycosis, Mycetoma, Nocardia brasiliensis, Osteomyelitis, Sporotrichoid nocardial mycetoma Introduction The genus Nocardia comprises gram-positive, aerobic, acid-fast, filamentous bacteria with a tendency to fragment into bacillary and coccoid forms. They are found worldwide and are saprophytes of soil, decaying wood, water, and air. Nocardia asteroides complex, N. brasiliensis, N. farcinica, and N. nova are commonly implicated for infection in humans.[1] N. brasiliensis is usually associated with subcutaneous infection, while N. asteroides causes more serious invasive infection presenting commonly as pneumonia in patients who are immunocompromised, have underlying chronic lung disease, or are on long-term steroid therapy. [2],[3] Dissemination to other organs, including skin and soft tissue, may occur. [3],[4] Traumatic inoculation in the skin is the typical mode for acquisition of infection in immunocompetent hosts, resulting in an acute inflammatory response terminating in necrosis and abscess formation; granuloma formation is uncommon. Cutaneous disease may thus manifest clinically as 1) acute superficial skin infection with abscesses or cellulitis, 2) mycetoma, 3) lymphocutaneous (sporotrichoid) infection, or 4) disseminated infection with skin involvement. [3],[1] Mycetoma, with the clinical triad of tumefaction, draining sinuses, and granules in the discharging pus, is characteristic and perhaps easy to diagnose clinically. Cultural isolation of the microorganism and species identification by various biochemical reactions or molecular techniques will be confirmatory. [5],[6] An early diagnosis, particularly for nocardial mycetoma cases, is important as drastic surgical measures such as deep tissue debridement or amputation are unnecessary if chemotherapy is used early. However, its clinical diagnosis is often delayed, particularly in non-endemic areas, for lack of clinical suspicion, diverse clinical presentations, and its simulation of other deep mycoses. This paper presents 4 clinical forms of this not so uncommon disease from a non-endemic region, emphasizing the importance of high index of clinical suspicion and repeated examination of exudates for Nocardia granules for an early diagnosis. Case Reports Case 1 A 32-year-old male laborer presented with swelling and multiple discharging sinuses over right ankle of 2 years′ duration that developed few days after an injury. A painful nodule developed at the injury site, which he frequently manipulated with thorns and needles; and progressively increasing painful swelling of the ankle ensued. Treatment with antibiotics, surgical debridement, and skin grafting at a peripheral center a year later did not benefit. Clinical examination showed diffuse, ill-defined, indurated swelling over medial side of ankle and intact grafted skin [Figure 1a]. It was studded with multiple, mildly tender, soft nodules; and a few sinuses having sero-purulent discharge or black crusts. Systemic examination and routine investigations, including complete blood counts, serum biochemistry, urinalysis, and chest x-ray films, did not show any abnormality. X-ray films of the foot showed osteolytic lesion in navicular bone. Skin biopsy revealed focal epidermal hyperplasia; chronic granulomatous inflammatory infiltrate comprising neutrophils, lympho-histiocytes and a few plasma cells; and fibroblastic and vascular proliferation. Periodic acid Schiff (PAS) and Ziehl-Neelsen (Z-N) staining were non-contributory. Repeated microscopy of sero-purulent material in potassium hydroxide (KOH) mounts showed multilobulated, vermiform grains [Figure 2A]. Skin biopsy specimens were submitted for histopathological examination and cultures on blood agar, Sabouraud′s dextrose agar (SDA) without antibiotics, and Lowenstein-Jensen (L-J) media. Aerobic culture on blood agar grew characteristic chalky white colonies of Nocardia spp. on the fourth day [Figure - 3]. Gram-stained smears from these colonies showed gram-positive, branching filamentous bacilli which were also weakly acid fast with modified Z-N stain, indicative of Nocardia spp. [Figure - 4], later confirmed to be Nocardia brasiliensis at National JALMA Institute for Leprosy and Other Mycobacterial Diseases, Agra (India), by standard biochemical tests, PCR-RFLP, and 16S rRNA sequencing. [5] He was put on treatment as recommended by Welsh et al. [7] and advised to follow up regularly. Case 2 A 29-year-old female agriculturist was hospitalized with multiple sinuses over the right leg of more than 2 years′ duration. History revealed that she had initially developed multiple, erythematous, minimally pruritic papular lesions, few having scanty purulent discharge, over right calf region. She did not recall any prior injury. She received intramuscular penicillin and anti-tuberculosis drugs from general practitioners without significant benefit. In the mean time, her lesions had increased. Cutaneous examination showed a diffuse swelling of right calf with multiple sinuses, some of them puckered and covered with adherent black-gray crusts [Figure - 5]. The swelling was warm to touch, indurated, mildly tender, had boggy feel and atrophic scars at places. Yellowish white pus discharging from a few active sinuses had no apparent granules. There was no regional lymphadenopathy. Findings from her systemic examination and routine investigations, including chest x-ray, were normal. X-ray films of the involved leg showed soft tissue swelling suggestive of thickened overlying skin, exudate collection in fascial planes, and normal underlying bones. Repeated microscopic examination of pus in KOH mounts showed typical vermiform granules with lobulated edges [Figure 2B]. Histopathology revealed mildly acanthotic epidermis, epithelioid cell granulomas with minimal caseation necrosis,a few Langhan′s giant cells in the mid-dermis, and no fungus in PAS-stained sections. Aerobic culture of the biopsy material yielded small chalky white colonies on blood agar at 35°C after 96 hours, identified to be of Nocardia spp. from gram-positive, weakly acid fast branching filamentous bacilli. Treatment with co-trimoxazole (sulfamethoxazole 800 mg + trimethoprim 160 mg / b.i.d.) and dapsone (100 mg/d) resulted in complete healing of all lesions with puckered scarring in a year. Case 3 A 71-year-old male laborer presented with multiple ulcers over left hand and forearm of 1-year duration. He had sustained a roadside injury over dorsum of left hand that healed following treatment from a general practitioner. Four months back, he developed painful swelling over left forearm with multiple sinuses and sero-purulent discharge. He was treated for tubercular osteomyelitis without benefit before his referral to us. Cutaneous examination showed diffuse swelling over dorso-medial aspect of left hand and an ill-defined, tender, indurated, lumpy swelling involving lower third of the left forearm [Figure 6A] and [Figure 6B]. Multiple discharging sinuses, some of them covered with brownish black crusts, were present in sporotrichoid pattern over these swellings. A few of these sinuses showed puckering and were fixed to the underlying structures. Blood-stained purulent material could be expressed from some of the sinuses but no grains were evident. Some puckered scars were also observed. Findings from systemic examination and routine laboratory investigations, including chest x-ray, were essentially normal. X-ray films of left forearm showed osteolytic and sclerotic changes in underlying bones [Figure 6C]. Histopathology revealed mixed suppurative and granulomatous inflammation. Repeated KOH mounts from purulent discharge showed characteristic grains [Figure 2C]. Aerobic culture on blood agar grew characteristic colonies on the fourth day identified to be of Nocardia spp. from weakly acid fast, gram-positive, branching filamentous bacilli fragmenting into coccoid forms. These colonies later displayed a characteristic dry appearance, orange pigment, and musty odor in 10 to 12 days. The organism tentatively identified as Nocardia spp. was confirmed to be Nocardia brasiliensis at JALMA Institute of Mycobacterial Diseases, Agra (India) . Treatment with Welsh′s regimen was started. He is under long-term follow-up. Case 4 A 31-year-old woman having low backache was referred from the orthopedic clinic for dermatologic evaluation of multiple, erythematous, tender nodular lesions in her right gluteal and lumbosacral regions. She had developed them about 10 years back a few days after incision and drainage of gluteal injection abscess. Nodules and pus-discharging sinuses kept on appearing over a period, extending over right paravertebral and lumbosacral regions. She had received routine antibiotic and anti-tuberculosis drugs at peripheral centers. Cutaneous examination showed tender, erythematous nodules in a sporotrichoid pattern over right gluteal, lumbosacral, and paravertebral area [Figure - 7]; and a few sinuses having serosanguineous discharge and creamy white granules. Findings from systemic examination were essentially normal. Routine hematology, serum biochemistry, and x-ray films of chest/lumbosacral spine showed no significant abnormality. A computed tomographic scan of lumbosacral spine demonstrated reduction in intervertebral disc spaces; degenerative changes in L3-4, L4-5, and L5-S1 discs; and lumbar vertebrae with mild sclerotic changes. There was no significant abnormality of the adjoining soft tissue. Microscopic examination of granules in KOH mounts and Gram-stained smears showed typical morphology [Figure 2D]. Directly stained smears from these exudates showed gram-positive, branching filamentous bacilli which were also weakly acid fast. Histology of skin biopsy showed chronic inflammation and multiple foci of PAS-positive organisms. Aerobic culture of the biopsy material on blood agar at 35°C yielded small pale white colonies after 3 days of incubation, identified to be of Nocardia spp . Treatment with co-trimoxazole (sulfamethoxazole 800 mg + trimethoprim 160 mg / b.i.d.) was started but she did not turn up for follow-up. Discussion Nocardial infections occur worldwide, particularly in tropical/subtropical environments. In epidemiologic surveys, the annual incidence of nocardiosis has been estimated to be 500 to 1000 cases in the US and 150 to 200 cases in France, with 36% being of cutaneous nocardiosis.[8],[9] In India the first report on N. brasiliensis infection appeared in 1964. [10] However, exact prevalence of primary cutaneous nocardiosis still remains unknown, and the relevant information mainly comprises case reports and small case series on mycetoma from different parts of the country. [11],[12],[13],[14] Himachal Pradesh, a small hill state of India, is situated at 30°N and 75°E in the western Himalayas. Though occasional cases of pulmonary and ocular nocardiosis, chromomycosis, and pheohyphomycosis have been reported, the state is recognized for being endemic to cutaneous sporotrichosis.[15],[16],[17],[18],[19] Differential diagnosis of chronic discharging localized disease in an extremity includes mycetoma, chromomycosis, blastomycosis, coccidioidomycosis, sporotrichosis, tuberculosis, botryomycosis, syphilis, yaws, and neoplasia. Mycetoma (Madura foot, maduromycosis) is a chronic, localized infection of the dermis and subcutaneous tissue with indolent swelling and draining sinuses The granules in the discharge are actually aggregates of microcolonies of the organism. More than 20 species of fungi and bacteria have been implicated as etiologic agents of mycetoma. Approximately 40% of cases are due to true fungi (eumycetoma), and 60% are caused by aerobic actinomycetes (actinomycetoma). [20] Nocardia brasiliensis and N. asteroids account for the infection in majority of the cases and follow mostly forgotten, traumatic implantation or contamination of a wound involving the limb (foot) in majority of the cases. [20],[21] Since the lesions are invariably triggered by injury, involvement of back, arm, leg (as in our patient), or thigh is unusual and reported infrequently. [22],[23],[11] Upper back particularly gets involved in persons habitually carrying wood or soiled sacks on the back. [21]Men/women 20 to 50 years of age, walking barefoot, and working outdoors in rural settings are particularly at risk. [20] More or less, all our patients had similar clinical features as well. Our case-1 developed mycetoma of left foot following an occupational injury. A high index of clinical suspicion would have prevented surgery in him especially since nocardial mycetoma of even of long standing (case-2) responds well to co-trimoxazole therapy. Progression to fibrosis, mutilation, and finally loss of function is rapid in actinomycotic/nocardial mycetoma cases. Bone involvement occurs infrequently. The notable bony changes include periosteal thickening, osteoporosis and osteolysis.[12] Apart from skin lesions, sclerosis of navicular bone was observed in our mycetoma foot patient (case-1), while sclerosis and cortical erosions suggestive of osteomyelitis were evident in our case-3. Both these patients showed adequate response to co-trimoxazole without surgical intervention. The lymphocutaneous (sporotrichoid) syndrome can be caused by a wide variety of microorganisms - Sporothrix schenckii, Mycobacterium marinum , Leishmania spp., and Nocardia spp. being the common ones. Clinical suspicion in such cases appears to be of paramount importance, especially where cutaneous sporotrichosis is endemic. Nocardial lymphocutaneous syndrome is uncommon and accounts for only one third of the cases, the majority being due to Nocardia brasiliensis. [2],[24] Though often observed in patients having concomitant immunosuppression, this variety has been reported in immunocompetent patients as well. [24],[25],[26],[1] At first glance, our case-3 appears to be of lymphocutaneous sporotrichosis due to lesions appearing after roadside injury and endemicity of nocardiosis in the region. However, we were skeptical of the diagnosis in view of puckered sinuses draining purulent material and severe bone involvement. Smears from wound drainage were diagnostic, which also signifies the importance of clinical suspicion and repeated smear examination in all such cases. Our fourth patient developed lymphocutaneous nocardial mycetoma following an injection abscess; a phenomenon that has been observed previously with primary cutaneous norcadiosis. [27] Although their observed association in her may not imply a causal relationship, the distribution of skin lesions around injection site and subsequently along the lymphatics, and absence of other predisposing factors were suggestive. The degenerative changes in the underlying vertebral bones/discs in our patient appear more to be due to long standing nature of the disease in her. Despite characteristic clinical features, all our patients remained undiagnosed for long, perhaps for want of clinical suspicion. To overcome the problem of delayed or no diagnosis, the investigative work-up guided by clinical correlation, a good biopsy, and repeated microscopy for granules in pus specimens need be emphasized. Timely initiation of an effective treatment is imperative for a favorable outcome, but the duration of therapy is uncertain. It must be for a prolonged period in view of relapses among considerable number of patients after shorter courses of therapy. Co-trimoxazole is the recognized first-line drug for nocardia infection. [1] The therapeutic regimen introduced by Welsh et al. [7] consists of intravenous amikacin 500 mg and co-trimoxazole (both in b.i.d. doses) for a period of 3 weeks followed by continuation of co-trimoxazole alone for another 2 weeks. This 5 weeks′ therapy makes 1 cycle, and most patients require at least 3 such treatment cycles followed by co-trimoxazole monotherapy for 1 to 1½ years. In patients with sulfa intolerance or in those who fail this mode of therapy, alternative treatment must be based on sensitivity testing. Minocycline, tetracycline, amikacin, dapsone, and amoxicillin-clavulinic acid, cephalosporins, and imipenem, alone or in combination, have been successfully used.[Figure 1b] References
Copyright 2008 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv08258f1.jpg] [dv08258f3.jpg] [dv08258f5.jpg] [dv08258f2.jpg] [dv08258f4.jpg] |
| |||||||||


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}