 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
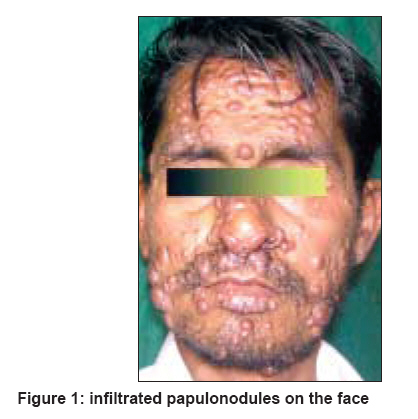
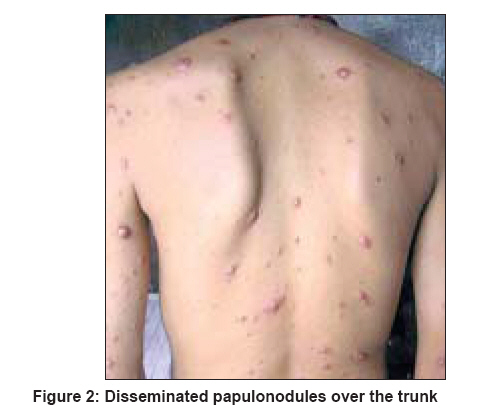
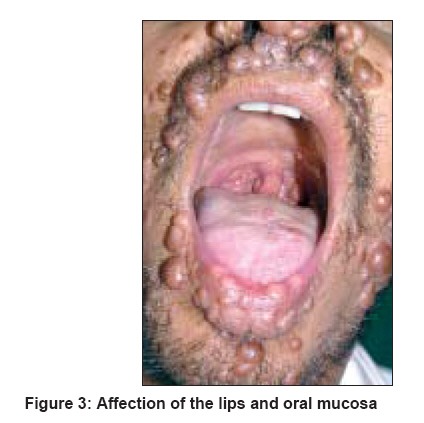
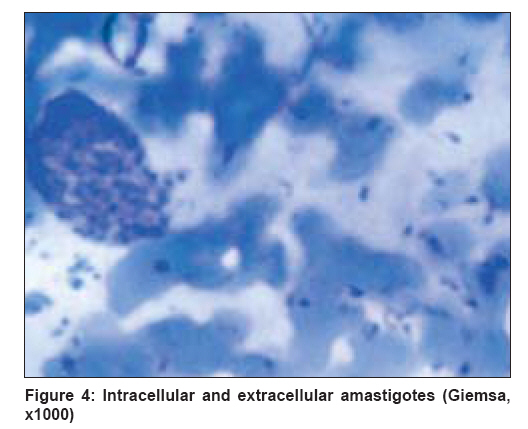
Indian Journal of Dermatology, Venereology and Leprology, Vol. 74, No. 6, November-December, 2008, pp. 641-643 Case Report Diffuse cutaneous leishmaniasis: Co-infection with human immunodeficiency virus (HIV) Chaudhary RajuG, Bilimoria FrenyE, Katare SK Department of Dermatology, Kesar SAL Medical College and Research Institute, Ahmadabad Code Number: dv08259 Abstract Cutaneous leishmaniasis is a disease caused by intracellular protozoal parasites belonging to the genus Leishmania. Immune suppression caused by HIV infection is an important factor for atypical presentation and widespread progression of cutaneous leishmaniasis. Diffuse (disseminated) cutaneous leishmaniasis and HIV co-infection is emerging as an extremely serious new disease. A 38-year-old HIV-positive man presented with a 12-month history of a progressive papule and nodular eruptions on face and extremities with infiltrations of nasal and oral mucosa. We report the case due to its atypical, widespread muco-cutaneous presentation masquerading as lepromatous leprosy.Keywords: Co-infection, Diffuse cutaneous leishmaniasis, HIV infection Introduction Human leishmaniasis is usually classified as visceral, localized or diffuse cutaneous, and muco-cutaneous.[1] CL can become disseminated (diffuse) in HIV-positive patients and is clinically characterized by multiple (>200), atypical, widespread infiltrations of skin lesions; and it weakens response to classic treatment. [2] Clinical diagnosis is confirmed by demonstrating amastigotes in Giemsa-stained smear and skin biopsy. HIV co-infected patients can be treated by various drugs like pentavalent antimonials, amphotericin-B, ketoconazole, miltefosine. [3],[4]Case Report A 38-year-old man hailing from Alwar district of Rajasthan, presented with a 12-month history of papulonodular lesions on face, trunk, and extremities with involvement of oral and nasal mucosa with hoarseness of voice. He also noticed fatigue, recurrent gastroenteritis, and remarkable weight loss since last 6 months. There was no past history of any major illness or prolonged fever with hepatosplenomegaly suggestive of kala azar. He gave history of multiple unprotected extramarital sexual contacts. Physical examination showed multiple, bilateral, asymmetrical, asymptomatic papulonodular lesions on face, trunk, and extremities [Figure - 1], [Figure - 2]. Infiltrations of oral and nasal mucosa were also found with involvement of tongue, soft palate, and posterior pharyngeal wall [Figure - 3]. There was no history of pain and pruritus, and there were no signs of ulceration and scarring. There was no lymphadenopathy and hepatosplenomegaly. Hepatic and renal functions were normal. Ultrasonography of abdomen was normal. He tested positive for HIV 1 by the ELISA and Western blot tests. The gp160, gp120, gp41, p24, p51 bands were present on western blot test. Blood counts and biochemistry values were within normal limits: Hb-11.8 g/dl; Total WBC - 5800 mm 3 ; P65, L29, E4, M2, B0; erythrocyte sedimentation rate - 18 at hr; serum bilirubin 1mg/dl; serum glutamate pyruvate transaminase (SGPT) - 35 U/L; serum creatinine - 0.7 mg/dl; blood urea - 25 mg/ml; and random blood sugar - 85 mg/ml. CD-4 T cell count was low (95/mm 3 ). Giemsa staining of scrapped materials from cutaneous lesions showed presence of 2-3 microns blue Leishman bodies [Figure - 4]. Skin biopsy from a single papular lesion revealed a massive dermal histiocytic infiltration with round cytoplasmic microgranules 1 to 2 microns diameter. The differential diagnosis of lepromatous leprosy was excluded by absence of hypo-aesthesia and negative Z-N stain of scrapped materials from lesions. The diagnosis of diffuse cutaneous leishmaniasis was established. We started ketoconazole 200 mg twice a day and referred the patient to an HIV specialist for antiretroviral therapy and further HIV care. Unfortunately he was lost to follow up after this. Discussion Leishmaniasis is one of the top five diseases targeted by the WHO Special Program for Research and Training in Tropical Diseases. About 1.5 million new cases are documented each year, and over 350 million people live in areas of active parasite transmission. [5] Leishmania species can cause a wide spectrum of cutaneous lesions in HIV-positive patients: localized cutaneous, mucosal, muco-cutaneous, diffuse cutaneous, or post-kala-azar leishmaniasis. [6] Clinical variants of leishmaniasis (cutaneous, mucosal, and visceral) and clinical status (subclinical, self healing, disseminated, death) are largely determined by parasite species and host cell mediated immunity (CMI) response. Several arguments suggest that dissemination of lesions is more determined by host immunogenic status (antigenic specific immunosuppression-IL-10 more than INF-Y) than by the virulence of the species involved. Recent publications have reported new or rare clinical variants of CL with or without HIV infection. The species involved in diffuse CL are Leishmania braziliensis, Leishmania amazonesis , and Leishmania aethiopica . In India, Leishmania donovani has been reported in post-kala azar dermal leishmaniasis (PKDL) associated with HIV. Leishmania pifanoi and Leishmania infantum have been found in CL with HIV co-infection. [7] Co-infection of HIV and leishmania, produces cumulative deficiency of the CMI, a key factor for primary protection against infection, recurrences, or metastasis of parasites. Such an HIV-infected patient has an atypical and severe clinical presentation of CL in terms of number (>200), sites and types of lesions (papulonodular). Mucosal lesions of CL in an HIV patient should not be considered as muco-cutaneous leishmaniasis (MCL) because parasites commonly disseminate and involve nasal and oral mucosa of body. [8],[9] Our case had multiple papulonodular lesions (>200) with widespread infiltration of the skin and nasal and oral mucosae. It differed from other forms of CL in which large numbers of lesions occur. These include PKDL, diffuse cutaneous leishmaniasis (DCL) and anergic cutaneous leishmaniasis. PKDL, in which cutaneous lesions accompany or follow visceral leishmaniasis caused by L. donovani, is mainly seen in India. PKDL was ruled out in our patient as he hailed from an area non-endemic for kala azar, there was no history of kala azar in the past, and there were no hypopigmented macules or hepatosplenomegaly or lymphadenopathy or any other sign of visceral leishmaniasis. DCL is characterized by large numbers (>10) of lesions like papules, nodules, or ulcers; and good response to classic treatment. Third, there was the anergic form, which was characterized by DCL secondary to underlying deficit in cellular immunity specific for certain species of leishmaniasis. The histopathological findings in dermatological lesions in diffuse CL and HIV co-infected patients are variable and can depend on immune status of the patients. In most cases, a large and even huge numbers of amastigotes histiocytes can be seen in dermal and subcutaneous tissue. Co-infection may amplify the immune defect against both leishmaniasis and HIV and increase disease severity and morbidity. Visceral leishmaniasis, 100-1000 times more common, is a major fatal outcome of co-infection. Diffuse CL in the absence of visceral involvement has been reported as a first manifestation leading to the diagnosis of HIV infection. CL in visceral leishmaniasis has been reported more commonly with HIV infection. [10] In India, there is high risk of mistaking diffuse cutaneous leishmaniasis for lepromatous leprosy especially since the latter is endemic here. We report the above case because of dual infection - cutaneous leishmaniasis and HIV - and the presentation of diffuse CL masquerading as lepromatous leprosy . References
Copyright 2008 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv08259f3.jpg] [dv08259f1.jpg] [dv08259f4.jpg] [dv08259f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}