 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
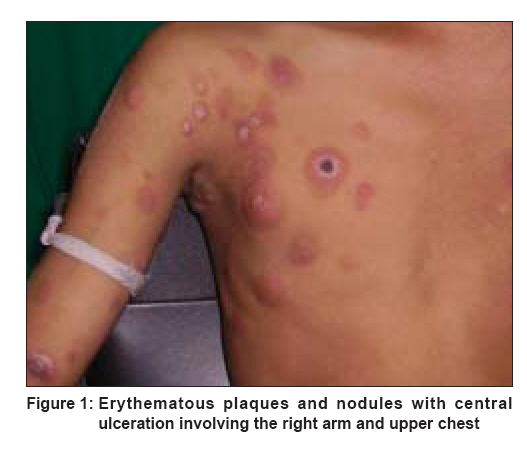
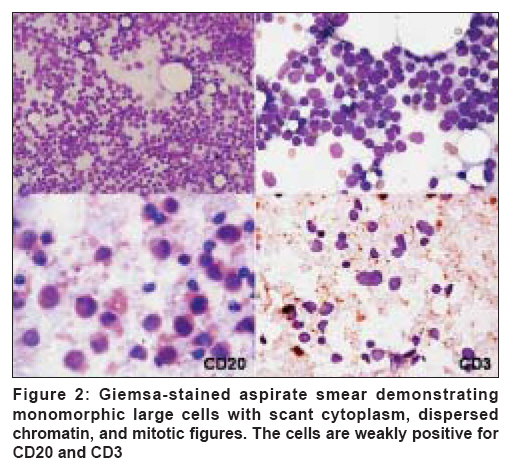
Indian Journal of Dermatology, Venereology and Leprology, Vol. 74, No. 6, November-December, 2008, pp. 652-654 Letter To Editor Primary cutaneous B-cell lymphoblastic lymphoma Gupta Ruchika, Borkataky Sangeeta, Aggarwal Deepti, Singh Sompal, Gupta Kusum, Kudesia Madhur Department of Pathology, Maulana Azad Medical College, New Delhi Code Number: dv08264 Sir, We recently came across a 14-year-old boy presenting with a 2-month history of multiple skin lesions, chiefly involving the trunk and both upper limbs. The first lesions appeared on the upper chest and grew progressively with spread to both arms and forearms. On examination, he had multiple cutaneous erythematous plaques and nodules, some showing superficial ulcerations. The nodules involved bilateral arms, forearms, and upper chest [Figure - 1]. There was no pallor, icterus, palpable lymphadenopathy, or hepatosplenomegaly. Chest radiography, abdominal ultrasound, computed tomography of chest and abdomen, and biochemical parameters were unremarkable. Fine needle aspiration cytology was performed from the cutaneous nodules on bilateral arms and chest. Giemsa-stained smears from all the 3 sites showed similar features. The smears were highly cellular, displaying a population of monomorphic cells dispersed singly. The cells showed scant basophilic cytoplasm, thin nuclear membrane, and finely dispersed chromatin with indistinct nucleoli. Occasional cells showed slight nuclear folding. Few mitotic figures were also identified [Figure - 2]. Background showed lymphoglandular bodies and a few histiocytes. With a presumptive diagnosis of lymphoma, immunocytochemistry was performed, which revealed weak positivity for CD20 (B-cell antigen) and negativity for CD3 (T-cell marker). Nuclear positivity for terminal deoxy-transferase (Tdt) was also seen. The cells were negative for CD99, synaptophysin, and desmin. Findings from hematological investigations, including peripheral smear, were within normal limits, and no immature cells were noted. Bone marrow aspiration and biopsy were also negative for immature cells in the marrow. In view of the clinical features and cytological findings, a diagnosis of primary cutaneous B-cell lymphoblastic lymphoma was rendered. The patient was treated with aggressive chemotherapy regimen. He attained complete remission and is currently disease free, 20 months after diagnosis. Lymphoblastic lymphoma (LBL), a neoplasm of precursor lymphoid cells, usually presents with a leukemic involvement (B-LBL) or as a mediastinal mass and/or lymphadenopathy (T-LBL). [1] Extranodal sites, including skin, breast, bone, central nervous system, gonads, liver, spleen, and bone marrow, have been reported to be involved. Cutaneous lesions in LBL have been reported in less than 20% of cases. In most of the cases, skin lesions are secondary to, or concomitant with, marrow or lymph node involvement. However, rarely, patients have cutaneous lesions as the presenting feature of LBL in the absence of nodal or marrow involvement, majority of these being T-cell type. [2] Primary cutaneous B-cell LBL has been reported in very few cases.[2],[3],[4] In some of the reports in the literature, the primary nature of the cutaneous lesions has not been definitely demonstrated. [2] In this report, the child presented with multiple skin lesions in the absence of marrow or lymph node involvement, thus validating the primary nature of cutaneous lesions. On pathological examination (biopsy or aspiration cytology), LBL shows a neoplastic population of small or medium cells with scant cytoplasm, round-to-oval nuclei with a thin nuclear membrane. Nuclear chromatin is fine, and numerous mitotic figures may be seen. Large pale macrophages containing nuclear debris may be present and may impart a starry-sky appearance to the lesion. [3] Histologic features do not allow distinction between T-cell and B-cell immunophenotypes, though presence of nuclear convolutions suggests T-cell type. For exact characterization, immunophenotyping is essential. [3] In our case, weak staining for CD20 suggested a B-cell immunophenotype, while cytomorphology was in favor of LBL. The differential diagnoses of LBL include the entire spectrum of ′small round blue cell′ tumors. Thus, LBL needs to be differentiated from Ewing′s sarcoma, Merkel cell carcinoma, neuroblastoma, rhabdomyosarcoma, Wilm′s tumor, neuroendocrine carcinoma, and metastatic small cell carcinoma. Lymphoid markers (LCA, CD20, and CD3) readily identify the lymphoid nature of the cells. Other immunohistochemical stains (cytokeratin, desmin, myogenin, chromogranin, synaptophysin, CD99) help in the distinction of LBL from other morphological mimics. At the same time, Burkitt′s lymphoma also needs to be excluded. Burkitt′s lymphoma tends to involve abdominal organs, and its cells possess coarse reticulated chromatin with several basophilic nucleoli and a thin rim of intensely pyroninophilic cytoplasm and distinct cell borders. [3] The prognosis of cutaneous LBL does not seem to differ from that of LBLs without cutaneous involvement, especially if aggressive chemotherapy is used. [5] In our case, a diagnosis of LBL was suggested on aspiration cytology, allowing for early institution of multi-agent chemotherapy, to which the patient responded very well and is in clinical remission after a follow-up of 20 months. In summary, we may state that we have herein presented a case of primary cutaneous lymphoblastic lymphoma of B-cell phenotype, which is a rare lesion. Fine needle aspiration cytology, assisted by immunocytochemistry, aids in an early diagnosis and institution of appropriate therapy and consequent rapid response. References
Copyright 2008 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv08264f1.jpg] [dv08264f2.jpg] |
| |||||||||

{kind=link}
{kind=link}