 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
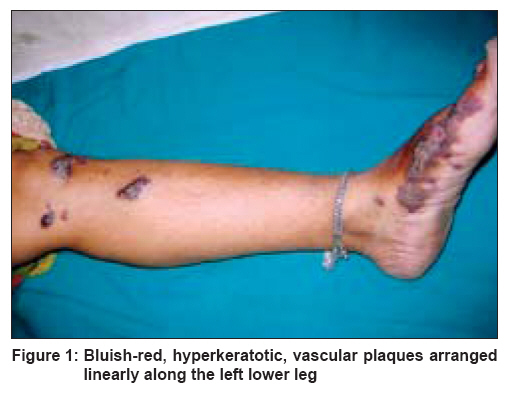
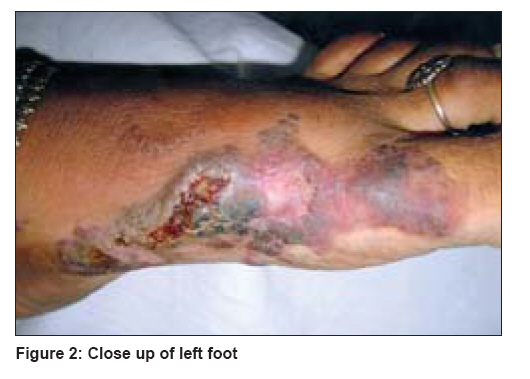
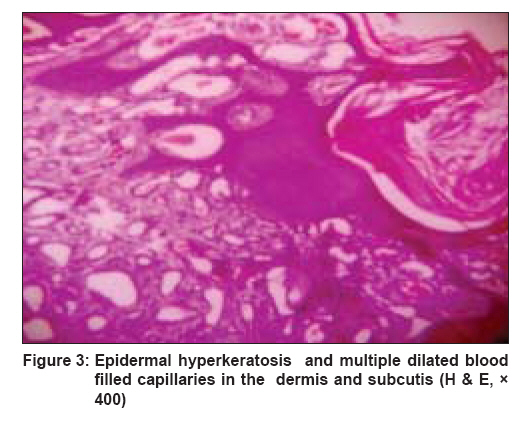
Indian Journal of Dermatology, Venereology and Leprology, Vol. 74, No. 6, November-December, 2008, pp. 656-658 Letter To Editor Linear verrucous hemangioma on the leg Jain VijayK, Aggarwal Kamal, Jain Sarika Department of Dermatology, Venereology and Leprology, Pt. B. D. Sharma Postgraduate Institute of Medical Sciences, Rohtak Code Number: dv08267 Sir, Verrucous hemangioma is a rare, congenital vascular malformation of the cutaneous and subcutaneous tissues with a predilection for the lower extremities. Although almost invariably present at birth, it may appear later or even in adult life. [1] The lesions appear as bluish red, well-demarcated, soft, and compressible swellings occurring on the legs in a great majority of the cases. Later on, they become verruciform and tend to enlarge and spread peripherally. Often misdiagnosed clinically as angiokeratoma or simple hemangioma, it is the distinct histopathology that helps to differentiate between these entities. [2] The linear or serpiginous form of verrucous hemangioma is extremely rare, and only a few case reports have been presented. [3],[4],[5] We herein report a case of linear variety which was localized to the leg. A 30-year-old woman presented with multiple bluish red verrucous lesions over the left leg [Figure - 1]. These lesions had been present from birth and had progressively enlarged, increased in number, and become more verrucous. It was the recurrent bleeding and infection in the lesions that caused the patient to seek medical advice. Dermatological examination revealed several well-circumscribed, hyperkeratotic, bluish red plaques of different sizes present in a linear distribution over the medial aspect of the left foot (including great toe) [Figure - 2] and extensor aspect of the left leg (including the knee). Surface of the lesions was verruciform and showed crusting at places. Few dark red macular lesions were present on and around the knee. Both the limbs were of equal length. Histopathological examination revealed epidermal hyperkeratosis and irregular acanthosis. Dermis showed numerous dilated thin-walled capillaries of various sizes extending down into the subcutaneous tissues [Figure - 3]. Few of the capillaries were congested with blood. A diagnosis of verrucous hemangioma was made. In 1937, Halter [6] first used the term ′verrucous hemangioma′ to describe the case of a 16-year-old boy presenting with a linear purpuric cluster of plaques extending from the right buttock to the toes. Since then, several studies have described similar lesions under a diversity of names such as angiokeratoma circumscriptum naeviforme, angiokeratoma circumscriptum, angiokeratoma corporis naeviforme, keratotic hemangioma, naevus vascularis unius lateralis, and naevus keratoangiomatosus. [2] The exact incidence is therefore difficult to determine. Verrucous hemangioma typically starts as a bluish red lesion with small satellites. After a variable number of years, the lesions take on a characteristic bluish black color and develop a verrucous surface. Secondary bleeding and infection are frequent complications, which often result in reactive papillomatosis and hyperkeratosis and thus the older lesions acquire a warty surface. [7] Usually the involvement is unilateral. [5],[8],[9],[10] Bilateral arrangement has been seen in one case only. [11] A linear or serpiginous arrangement of lesions has rarely been mentioned. [5] It is not known whether these lesions correspond to the lines of Blaschko, because only a few cases have been reported. [3],[4],[5] Clinically, the differential diagnosis includes angiokeratoma, Cobb syndrome, angioma serpiginosum, lymphangioma circumscriptum, verrucae, and pigmented tumors. The histologic appearance closely resembles an angiokeratoma, as both lesions show vascular spaces just beneath a papillomatous and hyperkeratotic epidermis. [12] However, in contrast to angiokeratoma, the vascular spaces in verrucous hemangioma also involve the lower dermis and subcutaneous tissues. In fact, verrucous hemangiomas are true vascular malformations; unlike angiokeratomas, which represent telengiectasias secondary to injury.
This case is being reported for the sheer rarity of its presentation. References
Copyright 2008 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv08267f1.jpg] [dv08267f2.jpg] [dv08267f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}