 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
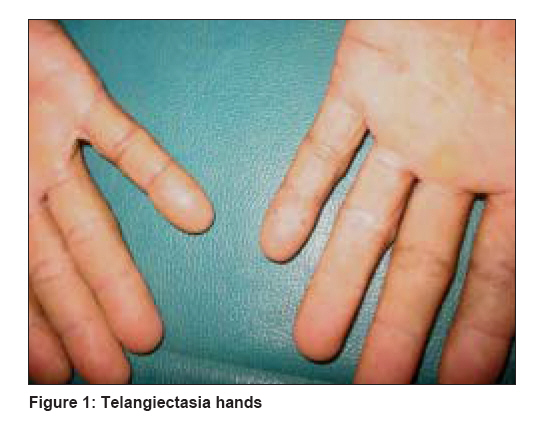
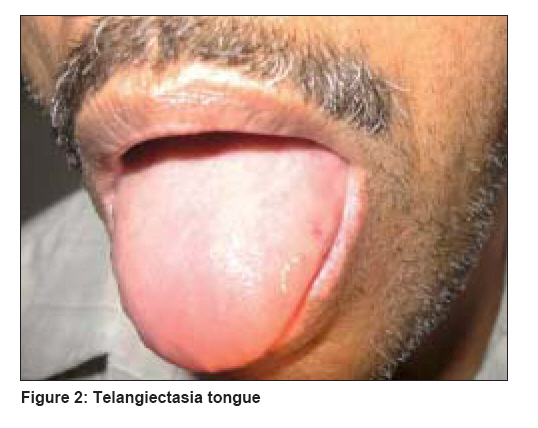
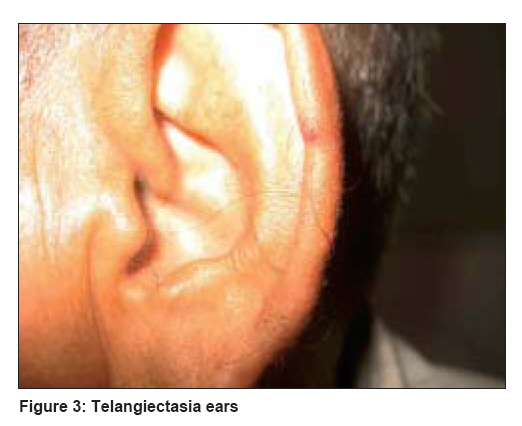
Indian Journal of Dermatology, Venereology and Leprology, Vol. 74, No. 6, November-December, 2008, pp. 659-661 Letter To Editor Osler-Weber-Rendu syndrome associated with vitiligo Kaliyadan Feroze Department of Dermatology, Amrita Institute of Medical Sciences, Kochi, Kerala Code Number: dv08269 Sir, A 60-year-old male patient presented to our outpatient department with a complaint of asymptomatic, depigmented lesions over his hands, feet, and lips of more than 10 years′ duration. The patient was a known diabetic on insulin. He had been evaluated and treated for the past 10 years for recurrent epistaxis. No apparent cause was found for the epistaxis. The patient also had a persistently low hemoglobin level, for which he had been on vitamin and iron supplements. Findings from all relevant investigations, including bone marrow biopsy, were normal. He gave no history of other bleeding tendencies. There was no history of hematemesis, hemoptysis, bleeding from the gums, or melena. On examination he was found to have acral vitiligo. Interestingly we found multiple telangiectasias over the hands, lips, tongue, and ear lobes [Figure - 1],[Figure - 2],[Figure - 3]. The patient had noticed these red lesions increasing in number over the last few years but had attached no significance to the same. Apparently all his brothers too had similar lesions over the extremities, but none had a history of epistaxis or other significant bleeding tendency. A skin biopsy confirmed the lesions to be telangiectasia. Based on the history and clinical findings, the possibility of Osler-Weber-Rendu syndrome was considered. The patient was extensively investigated including abdominal, chest, and neurological imaging, to rule out other systemic involvement. All findings were within normal limits. Osler-Weber-Rendu syndrome, or hereditary hemorrhagic telangiectasia (HHT), is easily recognized in individuals displaying the classical triad of epistaxis, telangiectasia, and a suitable family history, but the disease is more difficult to diagnose in many patients. In our case, we assume that the diagnosis was missed earlier probably because the lesions were few and not very evident initially. Serious consequences may have to be faced if visceral arteriovenous malformations (AVM), particularly in the pulmonary circulation, are unrecognized and left untreated. [1] The diagnosis of Osler-Weber-Rendu syndrome is essentially clinical. The 4 criteria (epistaxis, telangiectasia, visceral lesions, and an appropriate family history) are carefully delineated. The HHT diagnosis is definite if 3 criteria are present (which was so in our case). A diagnosis of HHT cannot be established in patients with only 2 criteria, but should be recorded as ′possible′ or ′suspected′ to maintain a high index of clinical suspicion. If fewer than 2 criteria are present, HHT is unlikely, although children of affected individuals should be considered at risk in view of age-related penetration in this disorder. [1] Mutations in 2 genes, endoglin (ENG) and activin receptor-like kinase 1 (ACVRL1 or ALK1), have been associated with HHT, [2] HHT1 is caused by mutations in endoglin gene mapping on chromosome 9q, and HHT2 is caused by mutations in ALK1 located on chromosome 12q. [3] In view of the high prevalence of pulmonary and cerebral AVMs, all patients with HHT should be screened for their presence, and relatives of patients with HHT should be investigated for presence of the disease. [4] This case is interesting because of the association between Osler-Weber-Rendu syndrome and vitiligo. To the best of our knowledge, there has been only one previous report of a similar association. [5] We assume this to be a coincidental association as there seems to be no other definite basis to associate HHT with vitiligo, though recently independent studies have suggested a common chromosomal link (chromosome 7) for both vitiligo and HHT. [6],[7] This case also highlights the importance of thinking of, and looking for, the possibility of Osler-Weber-Rendu syndrome in patients presenting with recurrent epistaxis without any other apparent cause. References
Copyright 2008 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv08269f3.jpg] [dv08269f2.jpg] [dv08269f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}