 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
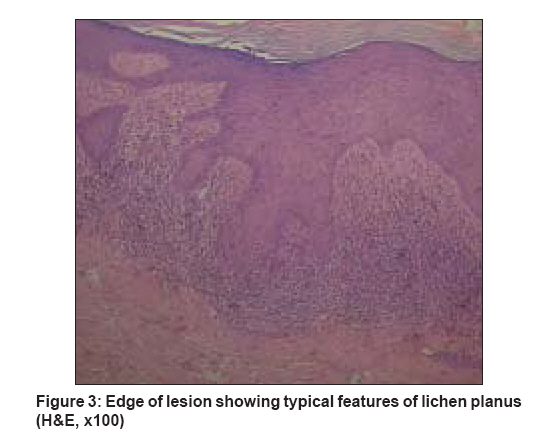
Indian Journal of Dermatology, Venereology and Leprology, Vol. 74, No. 6, November-December, 2008, pp. 662-664 Letter To Editor Basal cell carcinoma occurring in a lesion of lichen planus: Coincidence or causation? Bandyopadhyay Debabrata, Panda Saumya Consultant Dermatologist, BelleVue Clinic, Calcutta Code Number: dv08271 Sir, Cutaneous lichen planus (LP) is known to produce the rare complication (in less than 1% of cases) [1] of squamous cell carcinoma (SCC). The mucosal sites show particular predilection, and only certain variants of LP (chronic hypertrophic, ulcerative, atrophic, erosive) have demonstrated this complication until now. It is noteworthy that, till now, such transformation of any variant of LP into basal cell carcinoma (BCC) has not been reported. In this article, we report what is probably the first ever case of transformation of LP into BCC. A 74-year-old man presented with extremely itchy, widespread papular lesions of 20 years′ duration that had previously been clinically diagnosed and managed as LP. On presentation, he had a solitary facial lesion in the paranasal region that had become especially itchy over the past few weeks; and there was, reportedly, one recent episode of bleeding from the lesion following scratching. According to the patient, the facial lesion had been fairly persistent at the same site over the last two decades. The patient was a former sales professional who used to travel extensively. On examination, typical lesions of LP were present in a generalized distribution, with predominant involvement of lower limbs. The lesion in question was a darkly pigmented, indurated plaque (10 x 20 mm) on the left paranasal region [Figure - 1]. No lymphadenopathy or organomegaly could be discerned. The patient had no other complaints or associated physical problems. Findings from routine investigations, including blood counts, urinalysis, and blood chemistry panel, were within normal limits. Results of tests for human immunodeficiency virus (HIV) and hepatitis viruses were negative. Clinically, a neoplastic condition (including malignant melanoma) was considered to be a possibility. Full-thickness surgical excision with 10-mm margin on all sides was undertaken, and the tissue on histopathological examination showed unmistakable evidence of both LP and BCC; coexistence of both within a single field was observed [Figure - 2]. The BCC was of solid type with characteristic multiple lobules or islands of basaloid cells with peripheral palisading. Well-marginated lobules were separated from stroma by clefts. Melanin pigmentation was prominent in and around the tumor islands. Connection of the tumor lobules with surface epidermis [Figure - 3] could be discerned at places. Irregular acanthosis with saw-toothing of rete ridges was evident with dense, lichenoid, mononuclear infiltrate [Figure - 3]. Recovery of the patient after the surgery was uneventful. There has not been any recurrence since then. LP on the other sites has been quiescent with topical steroids and oral antihistamines. Malignant transformation of cutaneous LP is rare. Most of the reports till now have indicated involvement of the chronic hypertrophic variant, and invariably the transformation has resulted in SCC or its variants. Sites of chronic injury, irritation, or inflammation have long been known, albeit rarely, to develop into SCC. [2] That all the cases of LP with malignant transformation until now have had only SCC is thus not surprising. Lesions of actinic lichen planus may clinically resemble basal cell carcinoma in terms of having a thready rolled edge. [3] In addition, light (ultraviolet B (UVB) in case of BCC) is known to be involved in the pathogenesis of both conditions (actinic LP involving the face and basal cell carcinoma). This provides a window for BCC to occur in cases of longstanding facial actinic LP in terms of pathogenesis, though the same has not been seen in the past. With this background, it is essential to consider whether LP acted as a predisposing factor in the development of BCC in this case. In other words, is this case simply a coincidence (or co-localization) or is there any element of causation or predisposition? The unique characteristics of this case are occurrence in the eighth decade, history of chronic sun exposure, facial location, and persistence of the lesion at the same site for two decades. Constellation of these factors might have contributed to the occurrence of what is presumably the first documented case of LP transforming into BCC. Role of LP in the tumorigenesis could have some interesting connotations. It is known that susceptibility to UVB-induced inhibition of contact hypersensitivity is a better indicator of BCC risk than cumulative sun exposure, suggesting an important role for immune surveillance in protecting against development of cancer. [4] LP, being a chronic inflammatory autoimmune disease that produces basal cell damage, could result in a cytokine milieu that disturbs this surveillance mechanism. Still a question remains: why has there been no report of LP transforming into BCC hitherto? There has been some clinical evidence that individual proclivities to the development of BCC and SCC differ even within similar populations at risk.[5] There is increasing evidence as well that genetic factors play a role in the susceptibility of some individuals to BCC. It is probable that in our case any of these genetic mechanisms could have acted alongside the rare combination of favorable pathogenetic factors to result in the development of BCC. Unfortunately, cytokine profiling or genetic/clonality studies could not be done in this case due to lack of such facility. So the discussion on the moot question - co-localization or causation - has to remain speculative at this point of time, and both the possibilities remain open till more such cases are reported. This report should alert the clinicians about the possibility of malignant transformation of LP to BCC, particularly in the elderly population with longstanding unresponsive lesions of LP at sites prone to BCC (e.g., paranasal region, inner canthus). This awareness is particularly necessary at a time when we have a globally burgeoning population of the elderly and, at the same time, an increasing incidence of BCC worldwide. [6] References
Copyright 2008 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv08271f2.jpg] [dv08271f3.jpg] [dv08271f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}