 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
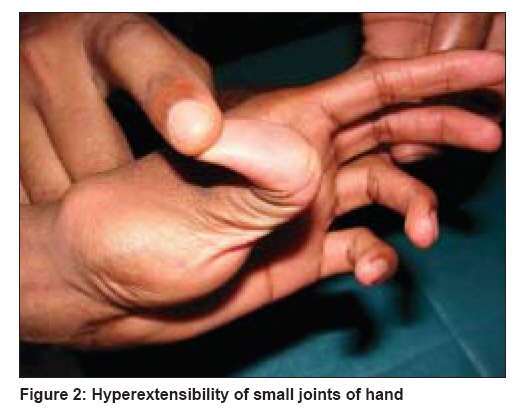
Indian Journal of Dermatology, Venereology and Leprology, Vol. 74, No. 6, November-December, 2008, pp. 664-666 Letter To Editor Type IV Ehlers-Danlos syndrome associated with factor VIII deficiency Kaliyadan Feroze, Namboothiri Sheela Department of Dermatology, Amrita Institute of Medical Sciences and Research Centre, Kochi, Kerala Code Number: dv08272 Sir, A 25-year-old patient was referred to us for itching and scaling over the scalp, face, and chest. The patient was at that time admitted for evacuation of a hematoma following a minimal trauma. The patient was a diagnosed case of factor VIII deficiency, with history of blood/clotting factor transfusions on several occasions. On examination there was minimal scaling and erythema restricted to the scalp, face, and chest. A clinical diagnosis of seborrheic dermatitis was made. Incidentally, on whole body examination, multiple healed scars were noticed on the patient′s body. Moreover, the patient had multiple varicosities over both lower limbs [Figure - 1] and significant hyper-elasticity of the skin and hyper-mobility of both large and small joints. On taking a detailed history regarding the same, the patient reported easy bruising, delay in wound healing, and excessive gaping of wounds since childhood. The patient mentioned that he was very good at ′break dancing′ because his joints were very flexible. There was no known family history of either easy bruising/bleeding disorders or joint hyper-mobility. There was no history of pneumothorax / pneumohemothorax, gastrointestinal involvement, tendon or muscle ruptures. The patient had been evaluated in various tertiary care centers for the last 15 years for his recurrent bruising tendencies. Except for a marginal low activity of factor VIII and a corresponding mild abnormal aPTT, his coagulation profile was normal. Based on this, he was labeled as a case of factor VIII deficiency and was treated on the lines of the same. His bruising tendency, however, did not show a significant response to the treatment. On examination we were able to demonstrate marked joint hyper-mobility, especially of the small joints of the hand [Figure - 2]. A positive Gorlin′s sign was also elicited [Figure - 3]. The patient′s skin also had a thin, translucent appearance. Other significant findings included a characteristic facies with thin lips and philtrum, a small chin, and a pinched nose. The patient also had a large hairy melanocytic nevus extending over his right arm and forearm. He also gave a documented history of an arteriovenous malformation adjacent to the site of the melanocytic nevus, which was excised earlier and apparently had taken a long time to heal. The patient was investigated considering a diagnosis of Ehlers-Danlos syndrome (EDS). The findings from ophthalmic examination were normal. Imaging studies, including MRI and scintigraphy, did not show any other significant hemangiomas / arteriovenous malformation. The patient was referred to the Department of Pediatric Genetics at our institution, where he was taken up for DNA molecular studies, and the specimens were sent to the University of Washington, Seattle, Washington. The DNA analysis demonstrated a mutation (C.1662 + 1G>T IVS24 + 1G>T) in one allele of COL3A1, the gene that encodes pro a 1(III) chains of type III collagen. The mutation results in the skipping of exon 24 and deletion of 18 amino acids in the pro a 1(III) chains encoded by the mutant COL3A1 allele. These molecular findings confirmed the diagnosis of EDS type IV. The findings from other blood investigations were normal except for the abnormal activated partial thromboplastin time (APTT) values (t- 41 seconds / c-31 seconds); prothrombin (PT) values were normal, and latest factor VIII activity result was 67.6%. Factor VIII assay was done earlier elsewhere had been persistently low. Virtually all of his symptoms can be explained on the basis of the type IV EDS. The prolonged APTT with a mild factor VIII deficiency, we believe, is just an association, which might have contributed to the severity of the symptoms. Unfortunately for the patient, the diagnosis of EDS was completely missed till the age of 25 years. EDS IV or the vascular type of EDS is an autosomal dominant disorder characterized by joint and dermal manifestations as in other forms of the syndrome, with proneness to spontaneous rupture of bowels and large arteries. The prevalence for all forms of EDS varies between 1/10,000 and 1/25,000, the EDS type IV representing approximately 5% to 10% of cases. The vascular complications may affect all anatomical areas, with a tendency for affecting arteries having large and medium diameter. [1] Superti-Furga et al. [2] provided the first description of a mutation in the COL3A1 gene in type IV EDS. Since then, many different types of mutations in the COL3A1 gene in EDS IV have been reported. It has also been known for a long time that different mutations affecting the stability and secretion of the pro alpha 1(III) chains of type III procollagen can be involved in EDS, suggesting that EDS type IV is biochemically heterogeneous. [3] Molecular analysis is essential for confirmation of EDS IV, even though a diagnosis can be made essentially on a clinical basis. There have been many reports of EDS associated with bleeding tendencies. This includes clotting factor deficiencies, Von-Willebrand′s disease, and platelet dysfunctions. [4],[5],[6] The exact basis for such an association is still not clear though. One of the points we would like to highlight through this case is the need to look for associated coagulation defects in cases of EDS. Though EDS is known to be associated with bruising, an underlying coagulation defect may accentuate the bruising tendency. In our case, interestingly, the coagulation defect, which we believe is only an incidental minor association, was identified early but unfortunately the EDS went undiagnosed for so long. Vascular EDS alone would explain the history of recurrent bruising and hematomas in the patient. Moreover, the factor VIII levels were always only marginally low, which could not explain the severity of his symptoms. Another interesting incidental association in our case was a larger hairy melanocytic nevus over the right upper limb. To the best of our knowledge this is the first case of type IV EDS, confirmed by molecular analysis, reported in Indian literature. References
Copyright 2008 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv08272f2.jpg] [dv08272f1.jpg] [dv08272f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}