 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
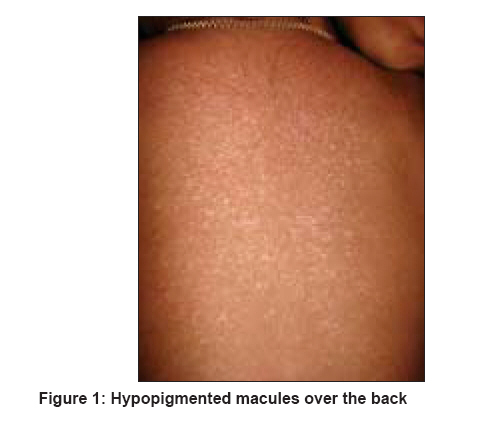
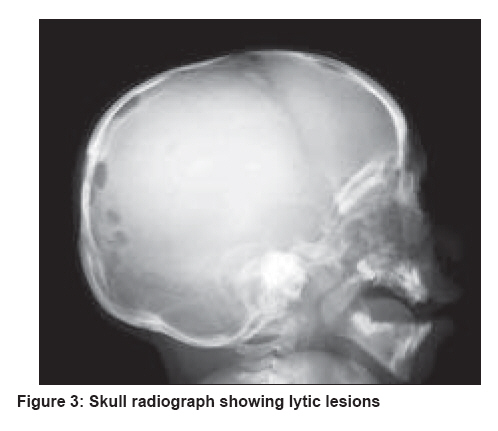
Indian Journal of Dermatology, Venereology and Leprology, Vol. 74, No. 6, November-December, 2008, pp. 670-672 Letter To Editor Langerhans cell histiocytosis presenting with hypopigmented macules Feroze Kaliyadan, Unni Manoj, Jayasree MG, Seethalekshmy NV Department of Dermatology, Amrita Institute of Medical Sciences and Research Centre, Kochi, Kerala Code Number: dv08276 Sir, A 3-year-old boy was referred to us by the oncology department for hypopigmented skin lesions, mainly over the upper back. The patient was being evaluated in the oncology department under the provisional diagnosis of Langerhans cell histiocytosis. The patient had presented to the oncology department with progressive proptosis associated with polyuria and polydipsia of 6 months′ duration. The hypopigmented skin lesions had been recurring since the age of 4 months, and the parents mentioned that the common sites affected were the face and the upper back. Skin lesions were asymptomatic. There was no history of any erythematous, vesicular, nodular, or ulcerative lesions. The patient had mild scaling of the scalp but no significant crusting or oozing at any stage. There was no history of any other significant skin or mucosal lesions. The patient had been on topical emollients for the skin lesions, and there was no definite history of topical steroids. The patient′s mother mentioned that the child had recurrent episodes of fever and upper respiratory tract infections, but had no significant weight loss or weakness. At the time of presentation, the patient did not have any significant respiratory or neurological symptoms. The child did not have a history of any spontaneous fractures or bone pains. On dermatological examination, the patient was found to have lesions mainly over the upper back and forehead, with scattered lesions over the front of his chest and neck. The majority of the lesions were hypopigmented macules with a few scattered skin-colored papules [Figure - 1]. There was mild scaling of the scalp but no significant involvement of the axilla or other body flexures. No evident purpuric, vesicular, pustular, nodular, or ulcerative lesions were seen. Mucosae and nails were normal. Langerhans cell histiocytosis (LCH) was the first possible clinical diagnosis considering the presence of proptosis, diabetes insipidus, and skin lesions. However, the nature of the skin lesions was not typical enough to suggest the possibility of cutaneous lesions of LCH; because though the lesions were mainly over the seborrheic sites with a few papular lesions, the majority of the lesions were hypopigmented macules. A skin biopsy taken from the hypopigmented macules revealed focal basal cell degeneration, exocytosis, and spongiosis. Papillary dermis showed infiltrate of histiocytes with folded nuclei, fine chromatin, and inconspicuous nucleoli admixed with lymphocytes and a few eosinophils. No significant mitosis was seen, and adnexal structures appeared unremarkable [Figure - 2]. Immunohistochemistry showed S-100 positivity in the histiocytic cells. The histopathology findings were consistent with the diagnosis of LCH. The one major limitation in our case was the lack of confirmation of LCH with CD1a or electron microscopy. However, we sincerely feel that the histopathological findings along with S-100 positivity, along with the typical clinical features like proptosis, diabetes insipidus, and the radiological changes, warrant a diagnosis of LCH. Other significant investigations included a bone marrow aspiration and biopsy, which revealed a normocellular marrow with trilineage maturation. Peripheral blood smear showed a picture of microcytic hypochromic anemia with thrombocytosis. CT scan showed multiple lytic lesions of the skull [Figure - 3] and soft tissue swellings in the orbit. Ultrasound abdomen revealed moderate hepatosplenomegaly. Based on the results of investigation, the patient was started on chemotherapy for multi-system LCH with vinblastine and prednisolone and is since under regular follow-up and treatment by the oncology department. For the skin lesions, the patient was put on topical emollients and mild steroids, with good improvement. No new skin lesions have developed since the patient was started on chemotherapy; however, the hypopigmentation has not completely subsided. Skin involvement is common with Langerhans cell histiocytosis (LCH), and up to 50% of cases with multi-system disease may initially present with a rash, the intertriginous zones and lumbosacral areas being the most commonly affected. [1] The common skin lesions described as part of LCH include vesiculopustules, seborrheic dermatitis-like rash, mucosal lesions (erosions, petechiae, and granulomas), erythematous papules, nodular ulcerative lesions, and generalized petechiae. [2],[3] Skin lesions in varicelliform pattern, with umbilicated vesicular lesions, have also been described. [4] Hypopigmented lesions have been described commonly in LCH as a sequelae following healing of papular or nodular lesions, especially in the context of congenital self-healing Langerhans cell histiocytosis (CSHLCH); [5] but to the best of our knowledge, hypopigmented macules histopathologically showing features of active LCH have not been described in multi-system disease. References
Copyright 2008 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv08276f1.jpg] [dv08276f3.jpg] [dv08276f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}