 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
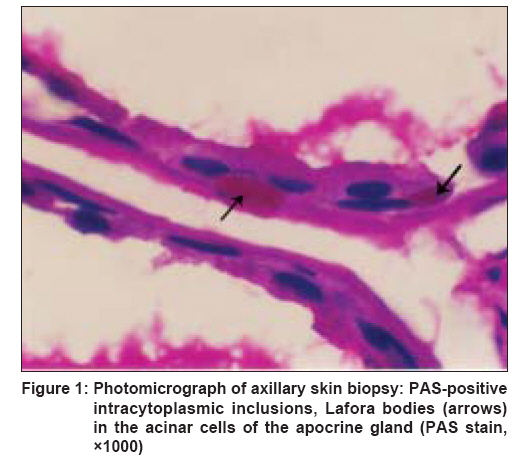
Indian Journal of Dermatology, Venereology and Leprology, Vol. 74, No. 6, November-December, 2008, pp. 672-673 Letter To Editor Lafora's disease diagnosed on axillary skin biopsy in 3 patients Malur PR, Davanageri RS, Bannur HB, Suranagi VV Department of Pathology, JNMC, Belgaum, Karnataka Code Number: dv08277 Sir, Lafora′s disease is a rare neurometabolic disorder resulting in progressive decline in mental function. It is one of the five major conditions which produce progressive myoclonus epilepsy. [1],[2] It is characterized by pathognomonic endoplasmic reticulum-associated polyglucosan accumulations. [3] The syndrome of classic Lafora′s disease was first described by Unverricht in 1891. [2] The disease usually commences between the ages of 11 and 18 years, with equal incidence in both the sexes. [1] The most common presenting feature is a single seizure followed by progressive myoclonus, generalized seizures, intellectual decline, and severe motor and coordination impairments. [4] Death usually occurs within 10 years, most commonly due to pneumonia or complications related to degeneration of the nervous system. [1] The diagnosis of Lafora′s disease is based on demonstration of intracytoplasmic inclusions called Lafora bodies. [2],[5] We have come across 3 cases of Lafora′s disease in which Lafora bodies were demonstrated in the axillary skin biopsy, which is the best diagnostic procedure according to our experience. Three male patients in their second decade (16, 17, and 16 years) presented with a history of generalized convulsions, which started in the 10 th , 12 th , and 14 th years respectively. The clinical features were almost similar in all the 3 cases. There was progressive development of weakness, incoordinated movements, and decrease in school performance. Impairment of recent and remote memory, registration, recall, attentiveness, and intelligence with progressive mental deterioration and total disability was noted. There was no nocturnal myoclonus. Upon reevaluation, similar family history was obtained in that the elder sisters in the first 2 patients, had died of a similar illness. The third patient did not give history of any affected sibling. On general physical examination, in the first case the boy was stuporous, dehydrated, and had bed sores. The other 2 cases did not reveal any significant abnormalities. Systemic examination was normal. No focal neurologic deficits were found. Reflexes were normal. On investigations, hematological parameters, biochemical parameters, and urine analysis were all within normal limits. Examination of cerebrospinal fluid was normal. X-ray of chest and skull showed no abnormalities. Electroencephalogram (EEG) showed bilateral diffuse low voltage, delta waves slowing with frequent generalized, multifocal spike discharges. Histopathological examination of the hematoxylin and eosin-stained sections of the skin biopsy taken from the axillary region demonstrated no discernible histopathological abnormalities. Periodic acid Schiff stain (PAS), with diastase, revealed presence of Lafora bodies which were round-to-oval intracytoplasmic PAS-positive, diastase-resistant inclusions within the acinar cells of apocrine [Figure - 1] and eccrine glands. The Lafora body inclusions in Lafora′s disease are found in neurons, liver, skin, bone, and muscle. In 1981, Carpenter and Karpati proposed skin biopsy as a convenient method of diagnosing Lafora′s disease by identifying Lafora bodies within eccrine ducts. Other authors have confirmed these findings. Lafora bodies have been noted in apocrine duct cells, dermal peripheral nerve bundles, and peripheral nerve inclusions in muscle biopsy specimens. [2] They are seen as concentric target-like laminations, 1 to 30 microns in diameter. They are PAS positive, diastase resistant, Alcian blue positive, and variably metachromatic with methyl violet or toluidine blue. [6] PAS staining of the inclusions has been seen with both paraffin and cryostat sections, rapid visualization being with cryostat sections. [2] Skin biopsy is a convenient and the least invasive method of establishing the diagnosis of Lafora′s disease. Despite the absence of cutaneous clinical findings, typical inclusions are present in eccrine duct cells and peripheral nerve of skin biopsies. [2] Andrade et al. favored skin biopsy outside the axilla for diagnosis of Lafora′s disease so as to eliminate the false positivity due to apocrine contents, as the apocrine glands are absent outside the axillary and genital regions and the eccrine duct cell Lafora bodies are unmistakable. [7] Doaei et al. found axillary skin biopsy to be more reliable to make definitive diagnosis of Lafora body disease. They found abundance of Lafora bodies in the epithelial and myoepithelial cells of ducts of sweat, apocrine, and eccrine glands from the biopsy at axillary site. [8] Despite advances in the genetics of Lafora′s disease, skin biopsy remains a primary diagnostic modality. [7] Skin biopsy taken from the axillary fold in all 3 of our cases showed PAS-positive intracytoplasmic inclusions in the acinar cells of both eccrine and apocrine glands. Though the Lafora body inclusions can be identified in the cells of various tissues of the body, skin biopsy is a more convenient, cost-effective, easier, and safer method. Axillary skin biopsy is diagnostic, for it has more number of apocrine and eccrine glands. References
Copyright 2008 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv08277f1.jpg] |
| |||||||||

{kind=link}