 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
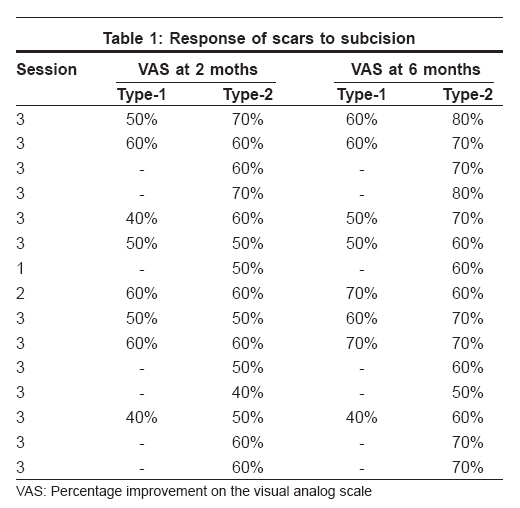
Indian Journal of Dermatology, Venereology and Leprology, Vol. 74, No. 6, November-December, 2008, pp. 677-679 Letter To Editor Subcision in rolling acne scars with 24G needle Vaishnani JigneshB Department of Dermatology, Surat Municipal Institute of Medical Education and Research, Umarwada, Surat-10 Code Number: dv08281 Sir, Post-acne scars are common and lead to cosmetic disfigurement of face. They are associated with social embarrassment and psychological problems. Post-acne scars [1] may be of different types and can be classified according to morphology into ice pick scar, rolling scar, and box scar. Treatment options depend on types of scars. Rolling scars are superficial, depressed, and atrophic; and they appear as shallow craters, resulting from fibrous anchoring of dermis to subcutis. Clinically, they appear as shallow, wide, rounded, or irregular craters. Margin is well defined, fibrous but essentially at the same level as that of surrounding normal skin. In 1957 Spangler reported use of bowmen′s iris needle to cut the fibrous strands beneath the deeply depressed facial scar. [2] The same technique was described by David Orentreinch and Norman Orentreinch under ′subcutaneous incisionless surgery′ in 1995. [3] Fifteen healthy patients with no history of keloidal tendency and no bleeding tendency and having depressed scars over face, cheeks, forehead, chin, nose, of varied dimensions, had undergone subcision therapy using 24G hypodermic needle, under aseptic precautions. Each scar was treated at intervals of 15 days. A maximum of 3 such sittings were carried out. Patients were followed up every week for possible results, as well as for early recognition of side effects, so further treatment was not carried out. Result was noted at end of 2 months and 6 months. All patients were followed up for a period of 6 months. In each patient, scars were classified as type-1 scar with fibrous margin [visibly and palpably thickened margin, which was raised above the surrounding normal skin] and type-2 scar without fibrous margin [margin essentially at the same level of surrounding skin]. Improvement was assessed by using visual analog scale [VAS] at 2 months and 6 months, and results were noted in terms of percentage improvement by calculating an average of percentage improvement on the basis of interviews of patient and his/her accompanying relatives. Out of the 15 patients, 9 were female and 6 were male, all between 20 and 25 years of age. The VAS improvement in scars ranged from 40% to 80%. All patients developed localized treatment-site edema and hematoma. Edema disappeared on the second day, and hematoma started resolving after the third day in all except 2 patients. Only 2 patients developed persistent hematoma - one after the first session of subcision, which resolved totally in around 4 months; and the other after second session of subcision, which resolved totally in around 3 months. None of the treated patients developed treatment-site infection, post-inflammatory pigmentary changes, or organized fibrous nodule. Results are shown in [Table - 1]. There was obvious clinical improvement in all patients treated with subcision for rolling scars, the improvement ranging from 40% to 80%; although persistent hematoma was encountered only in 2 out of the 15 patients, which resolved over a period of time without residue nodule or pigmentary changes. Improvement in type-2 rolling scars was slightly more than in type-1 rolling scars. This may be due to visibly abnormal fibrous margin of scar, which would not improve with subcision of undersurface of the rolling scar. Treatment of scar along with dissection [undermining] of surrounding fibrous margin was found to be superior to dissection [undermining] of scar alone. Cutaneous scaring is the end product of healing. The scar collagen fibers are usually smaller and more densely packed and often have high proportion of type-III collagen and fibronectin compared with surrounding normal skin. [4] Treatment of post-acne scars is a therapeutic challenge and requires multiple therapeutic modalities, as single modality alone is not hundred percent effective. Subcision is found to be an effective and economic tool for treatment of rolling scars of acne. [2],[3],[5] The subcision releases fibrous anchoring of dermis and the resultant hematoma together are responsible for the immediate clinical improvement in rolling post-acne scars. About 15% to 30% correction is expected in one sitting. After 5 to 10 days post-subcision, wrinkling of scar surface is obvious as hematoma starts resolving with continuous healing process. Wrinkling of scar surface is a good sign, and further possibility of organized hematoma is rare. Area of scar that appears tense should be undermined on subsequent subcision treatment. Subcision not only has a releasing effect on rolling scar but also produces trauma at microscopic level within scar tissues. Newer matrix and collagen tissue is laid down, which is responsible for permanent clinical improvement in depressed rolling scars. Scar remodeling is a continuous process, and it cannot be considered to be in a steady state until at least 2 years post-wounding. This may explain why results differ at 2 months and 6 months after subcision, and it suggests 5% to 10% improvement is likely beyond 2 months. [4] Subcision is not hundred percent effective; but unlike dermal fillers, which require subsequent injection after an interval of months, it gives permanent improvement in terms of correction achieved. Idea behind using 24G needles is that they are less painful and there is smaller hematoma formation compared to 18G to 20G needles; therefore, chances of post-subcision fibrous nodule are less; also, they are less traumatic, so unnecessary trauma to normal dermal tissue can be avoided. In conclusion, subcision is a minimally invasive, safe, permanently effective, and economical office procedure. Subcision is not hundred percent effective, and one should keep in mind the possibility of persistent hematoma and organized subcutaneous fibrous nodule as side effects. References
Copyright 2008 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv08281t1.jpg] |
| |||||||||

{kind=link}