 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
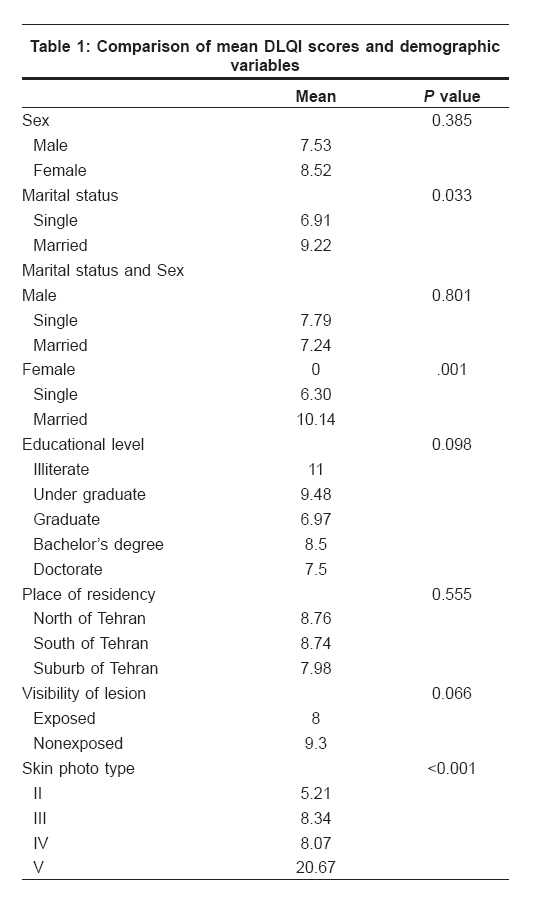
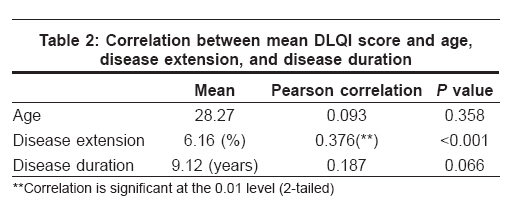
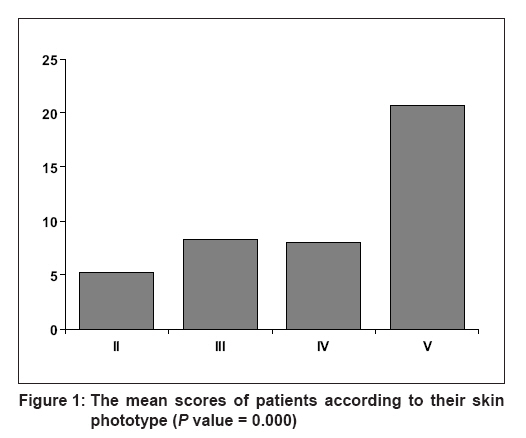
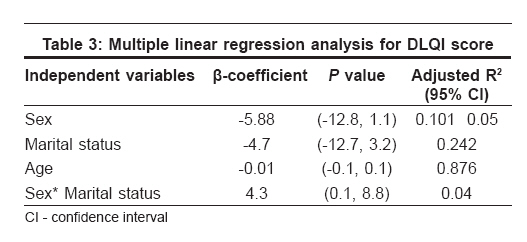
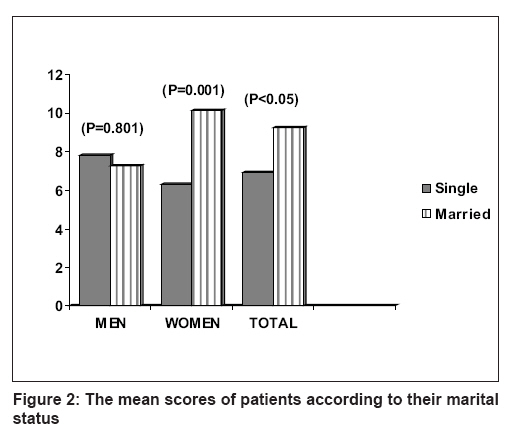
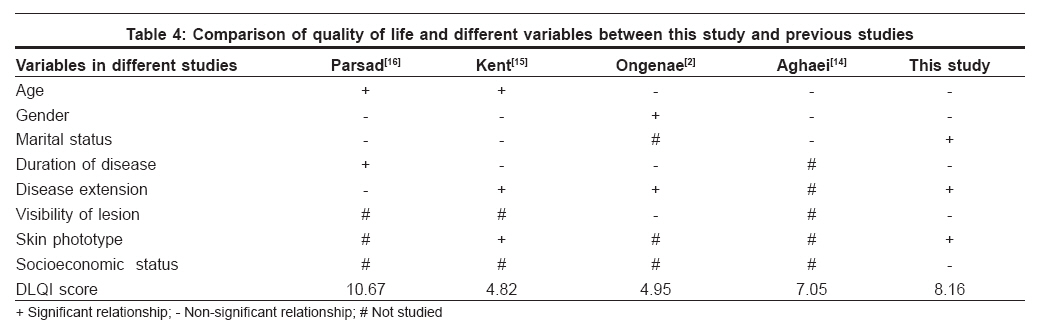
Indian Journal of Dermatology, Venereology and Leprology, Vol. 74, No. 6, November-December, 2008, pp. 700 Net Study Life quality assessment among patients with vitiligo: Comparison of married and single patients in Iran Dolatshahi Marjan, Ghazi Payam, Feizy Vida, Hemami MohsenRezaei Department of Dermatology, Tehran University of Medical Sciences, Tehran Code Number: dv08289 Abstract Background and Aims: Vitiligo is known to affect the quality of social and personal life in some countries. This study aims to assess the quality of life (QOL) in vitiligo sufferers among the Iranian population and to evaluate its relation with different variables. Keywords: Dermatology life quality index score, Quality of life, Vitiligo Introduction Vitiligo is a common, acquired, discoloration of the skin, characterized by well-circumscribed ivory or chalky white macules which are flush to the skin surface. [1] Vitiligo affects at least 1% of the total population. Although the disease does not produce direct physical impairment, it may considerably influence the psychological well-being of the patients. [1],[2] Since ancient times, patients with vitiligo suffered the same mental abuses as lepers; vitiligo was referred to as sweta kusth, meaning white leprosy. [3],[4] Appearance of skin can condition an individual′s self-image, and any pathological alteration can have psychological consequences. [5] Many vitiligo patients feel distressed and stigmatized by their condition. These patients often develop negative feelings about it, which are reinforced by their experiences over a number of years. Most patients of vitiligo report feelings of embarrassment, which can lead to low self-esteem and social isolation. [6],[7] The last decade has witnessed an increasing interest in the psychological effects of various skin diseases and the quality of life of patients suffering from these diseases. [3] The majority of studies on the psychological impact of vitiligo were conducted in USA and England. [2] On the other hand, in Iran, women with vitiligo face severe psychological and social problems; because according to Iranian legislature, if a woman has Baras (incorrectly translated as vitiligo) before marriage and does not inform her husband, the man has the right to divorce her without paying her what she could otherwise claim as her rights. [8] The purpose of this study is to show the burden of vitiligo on the quality of life of vitiligo patients among the Iranian population and identify variables that might predict poorer quality of life.Methods One hundred patients with vitiligo attending Razi Hospital, a postgraduate department of dermatology in Tehran, Iran, completed the questionnaire between January 2006 and December 2006. Because of the importance of obtaining a patient-based measurement of quality of life, [7],[9],[10],[11],[12] a widely validated questionnaire, the Dermatology Life Quality Index (DLQI) questionnaire designed by Finlay and Khan, [13] was used. Furthermore, reliability and validity of the Persian version of the DLQI questionnaire had been proved through a study in a group of Iranian vitiligo patients. [14] This dermatology-specific questionnaire is designed for use in adults, i.e., patients over 16 years of age. Moreover, it has the advantage of being short, easy to understand, and quick to complete; and it has also been used for several skin disorders. [2],[7] Patients above the age of 16 years with at least one vitiligo patch of whatever type were enrolled in this study. The patients were introduced to the subject of this study and informed about the personal nature of the questionnaire, and all those who gave their consent were given the questionnaire to be completed and returned to the dermatologist during the visit. The institutional ethical committee approved the study protocol. The questionnaire was classified into 6 headings: symptoms and feelings (questions 1 and 2), daily activities (questions 3 and 4), leisure (questions 5 and 6), personal relationships (questions 8 and 9), work and school (question 7), and treatment (question 10). Each question with 4 possible answers scored from 0 to 3. The DLQI score is calculated by summing the scores of all the questions, resulting in a maximum of 30 and a minimum of 0. [13] The higher the DLQI score, the more is the quality of life impaired. Other survey questions about demographic data, including age, gender, marital status, place of residency, educational level, and disease duration, were also answered by the patients. Dermographic data such as disease extension, visibility of lesion, and skin phototype (SPT) were collected by physical examination and observation. All statistical analyses were carried out using the statistical package for the social sciences (SPSS 11.5 for windows). Relation between DLQI score and each variable was assessed via one-way ANOVA, correlations and independent samples t-test, depending on the type of variable. Besides, in order to describe the relation between the DLQI score (as the response variable) and different explanatory variables, a multiple linear regression model was used. Results One hundred patients with ages ranging from 16 to 57 years filled out the questionnaire completely. The mean DLQI score of this studied population was 8.16 ± 5.423 (minimum = 0, maximum = 28). The results were summarized in [Table - 1] and [Table - 2]. There was statistically significant relationship between DLQI score and skin phototype. The mean DLQI scores in individuals with SPT-V were statistically higher than in those with other types ( P < 0.001). There was statistically significant, yet weak, relationship between disease extension and DLQI score ( P < 0.001, Pearson correlation = 0.376). There was a statistically significant relationship between DLQI score and marital status ( P = 0.033). The DLQI scores of single and married patients in each sex group were evaluated separately. Married women had significantly higher DLQI scores than single women ( P = 0.001), while single and married men showed no significant difference ( P = 0.801). There was no statistically substantial difference between the DLQI scores of male and female patients (36 males and 64 females, means = 7.53, 8.52 respectively, P = .385). There was no significant relationship between age and DLQI score statistically ( P = .358, Pearson correlation = 0.093). There was no notable relationship between the DLQI score and educational level of patients( P = .098). For this purpose we had divided the studied population into the following groups: illiterate, undergraduate, graduate, associate in art (A.A.), bachelor′s degree, master of science (M.Sc.), and doctorate There was no significant relationship between the DLQI score and place of residency ( P = .555). For this purpose the districts in Tehran are divided into 3 groups with regard to socioeconomic status: the districts which are located in northern Tehran have the highest socioeconomic status, the districts in the suburbs of Tehran have the lowest socioeconomic status, and the districts in southern Tehran have intermediate economic status. In this study 23 patients were from suburbs of Tehran, 17 patients were from northern Tehran, and 60 patients were from southern Tehran. There was no significant relationship between disease duration and DLQI score ( P = .066). There was no significant relationship between visibility of lesions and DLQI score ( P = .486). The variables which were correlated with mean DLQI score in univariate analysis significantly, had significant correlation with the mean DLQI score in multivariate regression analysis independently and separately as well (Skin phototype (SPT): P = .018 [Figure - 1]; disease extension: P < .001; marital status: P = .019). Moreover, to assess the concurrent effect of sex, marital status, and age on DLQI score, a linear regression model was utilized [Table - 3]. This analysis showed that there was a significant interaction with DLQI only between sex and marital status [Figure - 2]. Discussion The results of this study show that vitiligo had a profound effect on the QOL of patients in this study. The mean DLQI score (8.16) in the population of this study is higher compared to that in the studies by Finlay and Khan (7.2) [13] Kent, Al-abadie (4.82); [15] Ongenae et al (4.95) [2] and Aghaei et al, (7.05) [14] but lower than that in the study by Parsad et al (10.67). [16] Comparison of the QOL and different variables between this study and previous studies is shown in Table 1. There was statistically significant relationship between DLQI scores and SPT. People with SPT-V showed poorer QOL than those with other skin phototypes, which correlates with the finding by Kent et al. [15] This result can be due to the contrast between vitiligo lesions and darker skin, increasing disfiguration and drawing more attention. This may explain why the DLQI scores were found to be higher in the study by Parsad et al, which was conducted in India, a country with higher SPTs. Besides, there was a statistically significant relationship between the DLQI score and disease extension. In other words, patients with more disease extension showed poorer quality of life. The two latter results point out that the therapeutic strategies to reduce the number and extent of lesions and their disfiguring effects are definitely helpful. A significant relationship between DLQI score and marital status was found solely in this study and not in other studies. Married individuals showed a mean DLQI score of 9.22, meaning a poorer QOL compared to single patients, with a mean DLQI score of 6.91; whereas no significant difference had been found between single and married patients in previous studies. To find the reason for this result, we made a comparison regarding the quality of life between single and married persons within each sex group, separately [Table - 1],[Table - 3]. In fact, married and single men had no significant difference, while married women had a statistically notable higher score than single women. This posed the question, why is vitiligo so more worrisome in married women and how does it impact their QOL so significantly? The answer might be found in our special culture; also, according to our present legislature, if a woman has vitiligo before marriage and does not inform her husband, the man has the right to divorce her without paying her what she could otherwise claim as her rights for the divorce. [8] This is because vitiligo is incorrectly translated in Persian as Baras, while the correct equivalent for Baras is leprosy. According to the ancient book ′Kitab-fil-judham′ by Yuhanna ibn Masawayh (847 A.D.), Baras means ′white shiny′ and probably refers to leprosy in its early stages or in its tuberculoid form. [17] Yuhanna Ibn Sarabiyun (Serapion) (873 A.D.) described lepromatous leprosy as black Baras, while white Baras produced a whiteness of the skin. [17] According to the ancient book ′Canon′ written by Avicenna, which is perhaps the most famous medical textbook in existence, [17] vitiligo is not Baras because it does not infiltrate into profound tissues. The correct translated name of vitiligo is Bahak, which is limited to the superficial layers of skin. [18] In addition, we did not find any significant correlation between the DLQI score and age independently; this is consistent with the findings by Ongenae et al [2] and Aghaei et al. [14] On the other hand, there was no significant relationship between DLQI score and gender, which is consistent with most of the studies except the one by Ongenae et al [2] [Table - 4]. There was no significant relationship between DLQI score and educational level and place of residency independently. These two variables were considered indicators of socioeconomic status of individuals because there is no standard categorization of socioeconomic status in Iran. Therefore, it seemed that the socioeconomic status (a variable that has not been studied in previous studies) of this studied population did not affect the DLQI score significantly. There was no significant relationship between the DLQI score and duration of disease, which is in agreement with most of the studies except the one by Parsad et al. [16] We did not find any relationship between DLQI score and visibility of lesions, which is in agreement with the finding from the study done by Ongenae. [2] In other studies, the fact that the quality of life improves after the use of camouflage for disfiguring skin conditions suggests the importance of the visibility of lesions. [19],[20] It seems that because majority (90%) of our cases had exposed lesions and only 10% of them had exclusively unexposed lesions, the study′s sample population was not a suitable one to assess this variable. This study highlights major impact of vitiligo on the quality of life of patients and indicates specific groups of vitiligo patients who are at greater risk of experiencing poorer quality of life. Based on the results of this study, we can conclude that such patients require more aggressive efforts to cure this disease. Furthermore, it is critical to note the importance of psychological interventions, particularly in patients who experience poorer quality of life Finally, we wish to inform people that what the Islamic legislature refers to as Baras (incorrectly translated as vitiligo) is actually syphilis and leprosy, which are contagious diseases and were more worrisome in ancient times. Acknowledgments Our special thanks go to Professor Andrew Finlay for permitting us to use Dermatology Life Quality Index.References
Copyright 2008 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv08289t4.jpg] [dv08289t3.jpg] [dv08289f1.jpg] [dv08289t1.jpg] [dv08289t2.jpg] [dv08289f2.jpg] |
| |||||||||


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}