 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
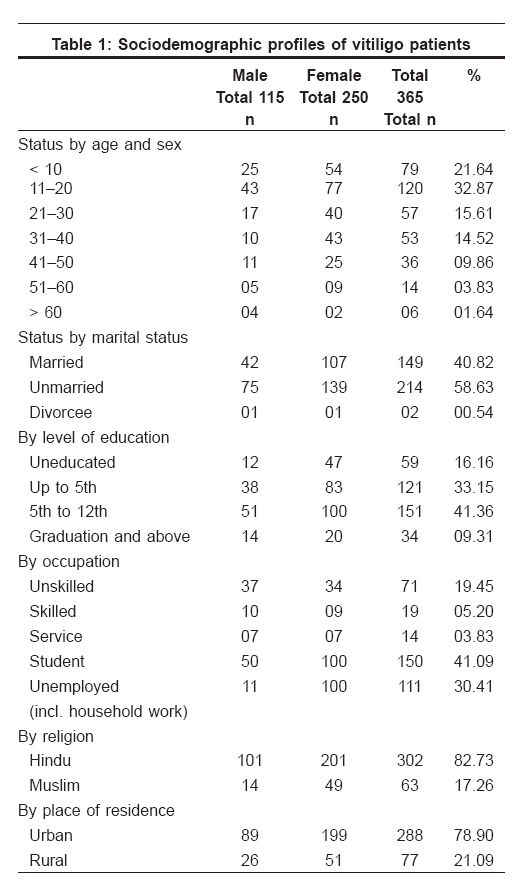
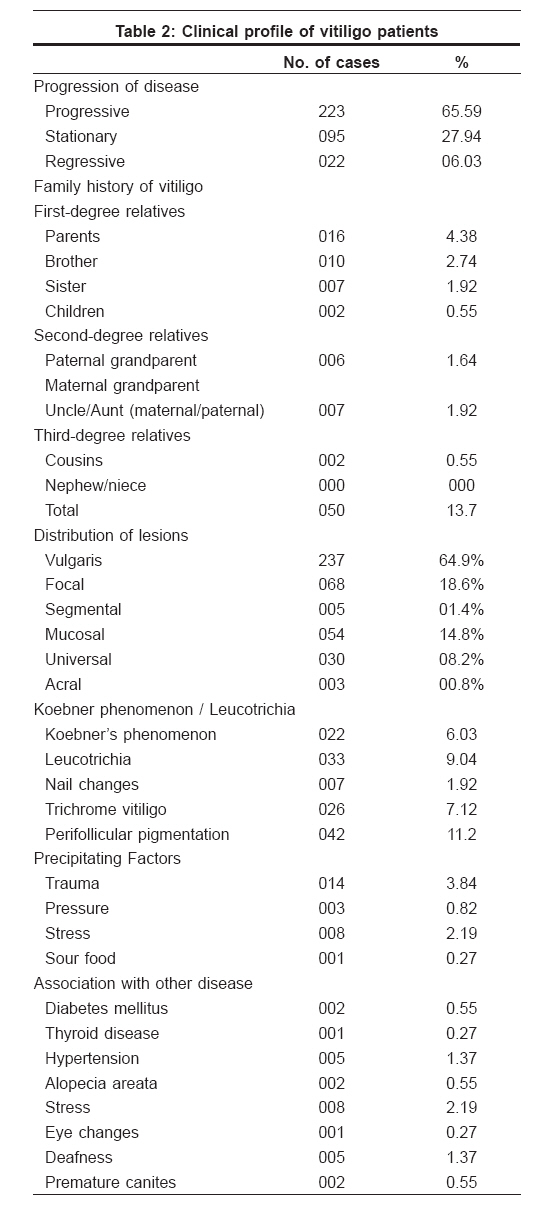
Indian Journal of Dermatology, Venereology and Leprology, Vol. 74, No. 6, November-December, 2008, pp. 701 Net letter Clinical and sociodemographic study of vitiligo Shah Hita, Mehta Anil, Astik Bhavesh Department of Dermatology, Venereology and Leprosy, Govt. Medical College, Bhavnagar Code Number: dv08292 Sir, Vitiligo is a common pigmentary disorder of the skin, with a worldwide incidence of 1%. [1] Widespread prejudices, ignorance, taboos, lack of scientific appraisal, and confusion of vitiligo with leprosy - all make it a social embarrassment for the patient, [2] although the patient′s life expectancy remains unaffected. [3] There is a stigma attached to vitiligo, and the families of the affected patients, particularly young females, are socially ostracized and the patients are considered unfit for marriage. [4] Some dermatological outpatient records show the incidence of vitiligo to be 3% to 4% in India although an incidence as high as 8.8% has also been reported. [5] In the Indian states of Gujarat and Rajasthan, the prevalence of vitiligo is very high being described by some as of epidemic proportions. [6] As Gujarat shows a high prevalence of vitiligo in India, the present study is an effort to learn more about precipitating factors and the clinical features of vitiligo patients in Bhavnagar, Gujarat. Methods The study was conducted over a 5-year period from May 2001 to May 2006. All new patients with vitiligo attending our OPD were included in the study; patients with depigmentation caused by chemicals, burns, or another disease were excluded. The diagnosis of vitiligo in all cases was made clinically. All the patients were interrogated for a detailed history, and a meticulous examination of each patient was carried out and recorded, giving special emphasis to the duration of the disease; marital status; precipitating factors; presence of leukotrichia, Koebner′s phenomenon, positive family history, and any other cutaneous or systemic illness. The sociodemographic profile of the patients was also recorded. Apart from routine blood and urine examinations, blood sugar and thyroid function tests were done whenever necessary. Lesions confined to one or a few patches localized in a particular area were grouped as focal vitiligo; lesions distributed in a segmental/dermatomal pattern, as segmental vitiligo; lesions noted over both face and acral regions, as acrofacial vitiligo; lesions affecting many parts of the body, as vitiligo vulgaris; and lesions confined only to mucous membranes, as mucosal vitiligo. [7] Results Incidence of vitiligo among new patients was 1.84%. A total of 365 patients were included in the study, out of which females (68.4%) were found to be more affected than males (31.6%), in a ratio of 2.1:1. The majority (32.82%) of the patients were in their second decade of life, and 58.63% of the patients were unmarried [Table - 1]. A positive family history was present in 50 (13.7%) patients. Trauma (3.84%) was the most common precipitating factor, followed by emotional upset (2.19%) and physical pressure (0.82%). History of progressive vitiligo was obtained in 65.59% of the patients [Table - 2]. Vitiligo vulgaris (64.9%) was the most common morphological pattern; other patterns seen were focal vitiligo (18.6%), acrofacial vitiligo (0.8%), mucosal vitiligo (14.8%), segmental vitiligo (1.4%), and universal vitiligo (8.2%). Leucotrichia was seen in 9% of the patients, and Koebner′s phenomenon was noted in 6% of the patients. The associated cutaneous diseases noted in our study were alopecia areata (0.55%), chronic urticaria (0.27%), and premature canitis (0.55%). Diabetes mellitus was found in 2(0.55%) patients; hypertension, 5(1.37%); hypothyroidism, 1(0.27%); epilepsy, 4(1%); and deafness, 5(1.37%). Discussion The prevalence of vitiligo is high in India, varying in the range of 0.46% to 8.8%. The different ethnic backgrounds of the population residing in different geographic regions with different environmental conditions may contribute to the wide variation in the prevalence of vitiligo in India. The female-to-male ratio in our study was 2.1:1, which is different from that reported by Handa and Kaur, Koranne et al., and Sarin et al. [7],[8],[9] Most of the reports showed that males and females were affected with almost equal frequency, but females outnumbered males in our study presumably because social stigma and marital concerns prompt women to seek early consultation. In 54.5% of the patients, the age at onset was in the first or second decade, consistent with most reports from India and the West. This shows that the disease starts at a younger age in the Indian population. However, Howtiz et al . [10] showed the age of onset to be between 40 and 60 years. There was a family history of vitiligo in 13.7% of our patients; first-degree relatives were affected in 35 patients. Vitiligo has a polygenic or autosomal dominant inheritance pattern with incomplete penetrance and variable expression. [11],[12],[13] Familial occurrence has been reported to be in the range of 6.25% to 30%. [14] Positive family history is considered to be a poor prognostic factor for vitiligo. A majority (65.59%) of our patients had progressive vitiligo at the time of presentation. Similarly, Dave et al. reported progressive vitiligo in 76% of the patients. [15] The majority (78%) of our patients were from urban areas, where environmental pollutants are more abundant. No significant difference was found between urban and rural residents according to a study by Lu Tao in China. [16] However, Slominski et al. point out that several environmental factors, including stress, extreme exposure to pesticides, sunlight, etc., have been implicated in the etiology of vitiligo. [17] No significant systemic illnesses were observed in our study. Autoimmune diseases were seen in 5 (1.36%) patients. The association of vitiligo with thyroid disease was 0.27% in our study but was reported to be 12% by Gopal et al. [18] Insulin-dependent diabetes mellitus is found in 1% to 7% of patients with vitiligo, [19] although it was seen in 0.55% of the patients in our study. To conclude, vitiligo was common in younger age groups in our study settings, with females of marriageable age forming the major group. A wide variety of clinical variations was noted in our study, but no significant systemic illnesses were recorded in our patients. References
Copyright 2008 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv08292t2.jpg] [dv08292t1.jpg] |
| |||||||||


{kind=link}
{kind=link}