
|
Indian Journal of Dermatology, Venereology and Leprology
Medknow Publications on behalf of The Indian Association of Dermatologists, Venereologists and Leprologists (IADVL)
ISSN: 0378-6323 EISSN: 0973-3922
Vol. 74, Num. 6, 2008, pp. 701-701
|
Indian Journal of Dermatology, Venereology and Leprology, Vol. 74, No. 6, November-December, 2008, pp. 701
Net Quiz
Hairy plaque on the thigh
Ustuner Pelin, Askin Ulku, Seckin Deniz, Ozen Ozlem
Department of Dermatology, Baskent University Faculty of Medicine, Ankara
Correspondence Address:Department of Dermatology, Baskent University Faculty of Medicine, 5. sokak, No. 48 Bahçelievler, 06490, Ankara, pelinustuner@hotmail.com
Code Number: dv08293
A 23-year-old woman presented to our institution with a solitary, slightly elevated, hairy plaque on the extensor surface of her left thigh. It had been present since birth and had gradually increased in size. She stated that after rubbing or scratching, the lesion would raise and harden temporarily; but otherwise, it was asymptomatic. The patient′s medical and family histories were unremarkable.
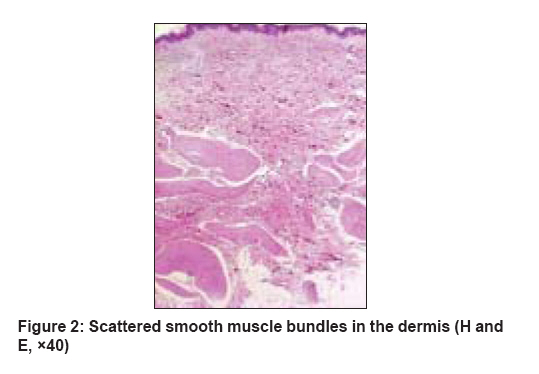
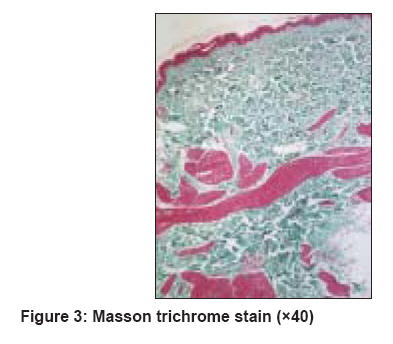
Physical examination revealed an ill-defined 10x5-cm skin-colored plaque with prominent overlying hairs and confluent, rubbery perifollicular papules [Figure - 1]. A 4-mm punch biopsy of the lesion was obtained and stained with hematoxylin-eosin [Figure - 2], and Masson′s trichrome [Figure - 3].
What is your Diagnosis ?
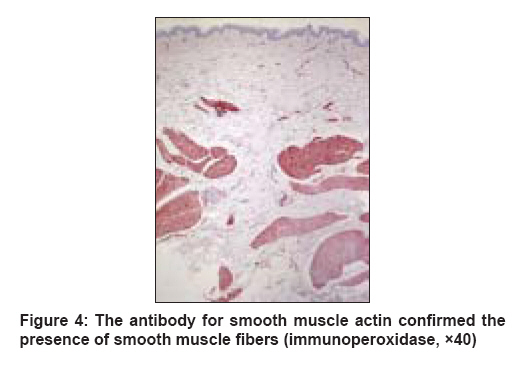
Diagnosis: Congenital smooth muscle hamartoma Histopathological examination revealed a normal epidermis and haphazardly distributed smooth muscle bundles in the reticular dermis. A thin retraction space around the bundles separating them from the adjacent dermal collagen also was observed [ Figure - 2]. The smooth muscle bundles were clearly seen with Masson′s trichrome stain [ Figure - 3]; these also stained positively with smooth muscle actin [ Figure - 4].
Discussion Congenital smooth muscle hamartoma (CSMH) is a skin-colored or lightly pigmented patch or plaque with hypertrichosis that originates from the smooth muscle fibers of the erector pili. It is often present at birth, with an estimated incidence of 1 in 2600 live births, but it also may be acquired. [1] It presents as a solitary lesion on the trunk or proximal extremities, with involvement of the lumbosacral area in two thirds of the patients. [2] Rubbing the lesional skin causes transient elevation or induration called the pseudo-Darier sign , which may be seen in 80% of the patients. [3] CSMH is characterized histologically by proliferation of smooth muscle bundles of the erector pili muscles in the reticular dermis. The pathogenesis is unknown. It may be due to the excessive proliferation of smooth muscle fibers at the time of maturation of the mesoderm during fetal life. [4] Abnormal proliferation of CD34-positive dermal dendritic cells is supposed to stimulate aberrant development of smooth muscle proliferation by releasing growth factors. [5]
The clinical differential diagnosis of CSMH includes congenital melanocytic nevus, Becker′s melanosis, solitary mastocytoma, leiomyoma, connective tissue nevus, nevoid hypertrichosis, and acquired localized hypertrichosis. [3] Differentiating CSMH from congenital melanocytic nevus is critical, as the latter, especially the giant congenital melanocytic nevus, may have a malignant potential. In congenital melanocytic nevus, a pseudo-Darier′s sign is not observed; and histopathologically, there is no smooth muscle proliferation in the dermis. In Becker′s melanosis, hyperpigmentation and hypertrichosis tend to increase with time; while in CSMH, these are not the predominant features, and they tend to decrease with age. Histopathologically, there is no smooth muscle proliferation in the dermis, and epidermal features such as increased pigment in the basal layer, acanthosis, elongation, and clubbing of the rete ridges are observed more frequently in Becker′s melanosis than in CSMH. Solitary mastocytoma and connective tissue nevus can be easily distinguished from CSMH by the presence of mast cell infiltration and increased dermal collagen respectively. Congenital smooth muscle hamartoma has a good prognosis with no reports of malignant transformation. Although no treatment is necessary, if the CSMH is cosmetically bothersome, surgical excision is the best option. Shaving, laser therapy, and chemical epilation are other treatment options. Diagnosis: Congenital smooth muscle hamartoma
Histopathological examination revealed a normal epidermis
and haphazardly distributed smooth muscle bundles in the
reticular dermis. A thin retraction space around the bundles
separating them from the adjacent dermal collagen also
was observed [Figure 2]. The smooth muscle bundles were
clearly seen with Masson’s trichrome stain [Figure 3]; these
also stained positively with smooth muscle actin [Figure 4].
DISCUSSION
Congenital smooth muscle hamartoma (CSMH) is a
skin-colored or lightly pigmented patch or plaque with
hypertrichosis that originates from the smooth muscle
fibers of the erector pili. It is often present at birth, with an
estimated incidence of 1 in 2600 live births, but it also may
be acquired.[1] It presents as a solitary lesion on the trunk or
proximal extremities, with involvement of the lumbosacral
area in two thirds of the patients.[2] Rubbing the lesional skin
causes transient elevation or induration called the pseudo-
Darier sign, which may be seen in 80% of the patients.[3]
CSMH is characterized histologically by proliferation of
smooth muscle bundles of the erector pili muscles in the
reticular dermis. The pathogenesis is unknown. It may be
due to the excessive proliferation of smooth muscle fibers at
the time of maturation of the mesoderm during fetal life. [4]
Abnormal proliferation of CD34-positive dermal dendritic
cells is supposed to stimulate aberrant development of
smooth muscle proliferation by releasing growth factors.[5]
The clinical differential diagnosis of CSMH includes
congenital melanocytic nevus, Becker’s melanosis, solitary
mastocytoma, leiomyoma, connective tissue nevus, nevoid
hypertrichosis, and acquired localized hypertrichosis.[3]
Differentiating CSMH from congenital melanocytic nevus
is critical, as the latter, especially the giant congenital
melanocytic nevus, may have a malignant potential. In
congenital melanocytic nevus, a pseudo-Darier’s sign is
not observed; and histopathologically, there is no smooth
muscle proliferation in the dermis. In Becker’s melanosis,
hyperpigmentation and hypertrichosis tend to increase with
References
| 1. | Zvulunov A, Rotem A, Merlob P, Metzker A. Congenital smooth muscle hamartoma: Prevalence, clinical findings, and follow-up in 15 patients. Am J Dis Child 1990;144:782-4. Back to cited text no. 1 [PUBMED] |
| 2. | Berger TG, Levin MW. Congenital smooth muscle hamartoma. J Am Acad Dermatol 1984;11:709-12. Back to cited text no. 2 [PUBMED] |
| 3. | Schmidt CS, Bentz ML. Congenital smooth muscle hamartoma: The importance of differentiation from melanocytic nevi. J Craniofac Surg 2005;16:926-9. Back to cited text no. 3 [PUBMED] [FULLTEXT] |
| 4. | Dupre A, Viraben R. Congenital smooth muscle nevus with follicular spotted appearance. J Am Acad Dermatol 1985;13:837-8. Back to cited text no. 4 [PUBMED] |
| 5. | Koizumi H, Kodama K, Tsuji Y, Matsumura T, Nabeshima M, Ohkawara A. CD34-positive dendritic cells are an intrinsic part of smooth muscle hamartoma. Br J Dermatol 1999;140:172-4. Back to cited text no. 5 [PUBMED] [FULLTEXT] |
Copyright 2008 - Indian Journal of Dermatology, Venereology and Leprology
The following images related to this document are available:
Photo images
[dv08293f3.jpg]
[dv08293f2.jpg]
[dv08293f1.jpg]
[dv08293f4.jpg]
|

{kind=link}
{kind=link}
{kind=link}
{kind=link}