
|
Indian Journal of Dermatology, Venereology and Leprology
Medknow Publications on behalf of The Indian Association of Dermatologists, Venereologists and Leprologists (IADVL)
ISSN: 0378-6323 EISSN: 0973-3922
Vol. 75, Num. 2, 2009, pp. 119-125
|
Indian Journal of Dermatology, Venereology and Leprology, Vol. 75, No. 2, March-April, 2009, pp. 119-125
Review Article
Targeted phototherapy
Mysore Venkataram
Centre for Advanced Dermatology, Bangalore
Correspondence Address:Venkat Charmalaya - Centre for Advanced Dermatology, 3437 1st G cross 7 main Subbanna Garden, Vijay Nagar, Bangalore - 560 040
mysorevenkat@hotmail.com
Code Number: dv09038
Abstract Phototherapy is one of the most important therapeutic modalities in dermatology. This field has seen several major advances in the recent years, the most recent being targeted phototherapy. Targeted phototherapy, which includes laser and nonlaser technologies, delivers light/laser in the ultraviolet spectrum, of specific wavelength, specifically targeted at the affected skin and thereby avoids many of the side effects of conventional phototherapy. The treatment has been claimed to be effective, quick, and needing fewer treatment sessions. The article reviews this new mode of phototherapy.
Keywords: Excimer laser, excimer light, phototherapy, psoriasis, targeted phototherapy, vitiligo
Introduction
Phototherapy is used for a wide variety of skin diseases. There has been considerable progress in cellular and cutaneous photobiology leading to improved understanding of different photodermatoses and their treatment. However, the developments in phototherapy have been comparatively slow, as reflected in a recent publication that "developments in phototherapy have not kept pace with scientific progress, as has been the case with radiotherapy" [1]
Nevertheless, the last two decades have seen significant technological advances, expanding the options while treating a patient who needs phototherapy [Table - 1]. The most important of these advances have been narrowband ultraviolet B (UVB) (311 nm) phototherapy and, more recently, targeted phototherapy [2],[3],[4] This article reviews the subject of targeted phototherapy in the light of the author′s experience during the last 4 years.
Disadvantages of Conventional Phototherapy
Conventional phototherapy consists of delivery of light energy by tube lights to the affected area. [3] Different machines used for this purpose include whole body cabinets, hand and foot machines, scalp machines, etc. These machines have the following disadvantages:
- Exposure of uninvolved areas
- Slow delivery system and lengthy treatment sessions
- Multiple and frequent visits to clinic
- Difficulty in treating certain areas (such as genitalia, oral mucosa, ear, etc)
- Difficulty in treating children who may feel intimidated by the large machines
- Large office space required to house the bulky machines
A new technique called targeted phototherapy which seeks to overcome these disadvantages has now become available [3],[4],[5],[6] Also called concentrated phototherapy, focused phototherapy, microphototherapy, this modality involves application of light energy directly focused on, or targeted at, the lesion through special delivery mechanisms such as fiber-optic cables. The term ′targeted phototherapy′ includes different technologies such as excimer laser, intense pulse light systems, and UV light sources with improved hand-held delivery systems.
Advantages of Targeted Phototherapy Several advantages have been claimed for targeted phototherapy: [5]
- Exposure of involved areas only and sparing of uninvolved areas, thus minimizing acute side effects such as erythema and long-term risk of skin cancer over unaffected skin
- Quick delivery of energy and thereby shortened duration of treatment
- Delivery of higher doses (super-erythemogenic doses) of energy because uninvolved areas are not exposed, higher doses of energy can be delivered selectively to the lesions, thereby enhancing efficacy and achieving faster response
- This has been claimed to shorten duration of treatment, leading to less frequent visits to clinic, and thereby lessen the inconvenience for the patient
- The maneuverable hand piece allows treatment of difficult areas such as scalp, nose, genitals, oral mucosa, ear, etc.
- Easy administration for children as delivery is hand-held
- Targeted phototherapy machines occupy less space
However, targeted phototherapy devices have certain disadvantages; they are more expensive. Also, they are not adequate to treat extensive areas in view of the cost of treatment and time involved in treatment. They are not recommended for use if lesions occur over more than 10% of the body area. [5]
Mechanisms of Action Most targeted phototherapy devices (laser or nonlaser type) emit radiation in the UVB range, with peak emission in the narrowband wavelength (around 308-311 nm), while some light-based nonlaser machines emit UVA radiation also. Hence mechanisms of action of targeted phototherapy systems are similar to those in conventional UVB/UVA therapy. [7],[8],[9],[10] UV light has been shown to have several effects on both epidermal and dermal cells, which explains its efficacy in treatment of cutaneous diseases such as psoriasis, vitiligo, and lymphoma. UVB radiation has been previously shown to induce DNA damage and pyrimidine dimer formation. Apoptotic mechanisms may be involved in the destruction of susceptible epidermal and dermal cells by UV light. UVB radiation has several effects on skin, such as induction of alteration in cytokine production, local immunosuppression, stimulation of melanocyte-stimulating hormone, increased melanocyte proliferation, and melanogenesis. UVB radiation also enhances production of vitamin D metabolites, which stimulate melanogenesis. UVA radiation may also produce similar effects. Targeted phototherapy may induce all these effects in a more aggressive way, because of delivery of supererythemogenic doses of radiation. [4],[5],[6] It has also been suggested that their enhanced efficacy may be due to their ability to deliver the energy to deeper dermal levels, and targeted therapy may therefore affect hidden target cells such as melanocytes. [6]
Different Types of Targeted Phototherapies As mentioned earlier, targeted phototherapy may be achieved by different sources such as laser (excimer), IPL (excimer light), and UV light [Table - 1].
Excimer Laser
First used in medicine for its ability to produce cold tissue ablation, excimer laser found applications in cardiology, ophthalmology, orthopedics, and dermatology [4] The word ′excimer′ refers to ′excited dimer.′ These lasers operate in the ultraviolet range, and examples include the 193-nm argon-fluoride; 248-nm krypton-fluoride; 351-nm xenon-fluoride; and of particular interest to dermatology, the 308-nm xenon-chloride laser. These lasers utilize a mixture of a noble gas and a halogen as a lasing material. The pulse repetition rate of the laser can be set up to 200 Hz with 3 mJ/cm 2 of energy per pulse. A pilot study in 2002 [6] showed significant benefits in vitiligo. Twenty-nine patches of vitiligo from 18 patients were treated 3 times a week for a maximum of 12 times with excimer laser, with parameters 120-nanosecond, 20-Hz pulse with a 10x10-mm spot size and a power output of 60 mW of laser light. Exposure time was 2 seconds, increased by 2 seconds at every other visit. Twenty-three vitiligo patches had 6 treatments, with some repigmentation in 57% of the treated patches. Eleven vitiligo patches from 6 patients had 12 treatments, with some repigmentation in 82% of the treated patches. Lesions which were previously resistant to treatment with other modalities also responded to excimer laser. The study concluded that "the degree of repigmentation in a period of 2 to 4 weeks is much higher than that achieved with any other present vitiligo therapy. The xenon-chloride excimer laser may represent a new treatment modality for the management of stable vitiligo". These results were confirmed by other studies, which showed benefit with excimer laser in patients of localized vitiligo who had been unsuccessfully treated with other modalities of treatment. [11]
In psoriasis too, the efficacy of excimer laser has been confirmed by several reports [12],[13],[14] Localized resistant lesions of psoriasis over elbow and knees were reported to be cleared in as few as 1 to 3 exposures, with moderately long remission. [12] Scalp psoriasis was also shown to respond well. [13] In another study which studied patient satisfaction, 55% of patients reported overall satisfaction and 25% reported that laser treatments were better than any other treatment they had tried. [14] Side effects reported, though usually mild, included burning pain during and after treatment, severe erythema, and blistering of skin. [14]
Excimer laser has been reported to be effective in other dermatoses also, such as oral lichen planus, [15] alopecia areata, [16] atopic dermatitis, [17] mycosis fungoides, and lymphomatoid papulosis. [18] Interestingly excimer laser has been found to be effective in hypopigmented striae [19],[20],[21] and hypopigmented scars, [19] conditions generally considered difficult to treat. Increase in melanin pigment, hypertrophy of melanocytes, and an increase in melanocytes within striae, leading to darkening of striae, were reported after use of excimer laser. [18] These results, if confirmed by larger data, will open up exciting new avenues for treatment of these important and common cosmetic problems.
After a period of initial excitement, subsequent studies have led to a reappraisal of the role of excimer laser in psoriasis [22],[23] and vitiligo [24],[25] Comparison of excimer laser, excimer lamp, and 311-nm narrowband UVB in patients with psoriasis showed similar clearance and no statistically significant difference in results after 10 weeks of treatment. [22] The study did show enhanced clearance rate in the laser group of patients when treated by an accelerated scheme of administration, but these patients also had higher rate of side effects such as blistering and crusting. The study concluded that "the only advantage of laser seems to be the ability to treat exclusively the affected skin and with a reduced cumulative dose, thus perhaps reducing the long-term risk of carcinogenicity" A large study of 140 patients with vitiligo treated by excimer laser showed excellent results in UV-sensitive areas, while UV-resistant areas such as acral lesions and lesions in joint areas responded poorly. [24]
Excimer laser machines have been introduced by companies such as Photomedex and Wave Light Technologies. However, the machines had several disadvantages such as high cost, huge weight and bulk, and difficulties in maintenance. These factors and the less-than-impressive data stated earlier justify the observation by James Fergusson that "in both theory and practice, this treatment is effective and the excimer 308-nm laser effected faster clearance at a lower cumulative dose and spared unaffected skin from unnecessary exposure. The blistering response may raise a problem for patients. Controlled trials are needed. I suspect that until such information is available, this expensive, high-tech treatment will remain confined to specialist centres". [26] This indeed has been the case and despite its introduction in 2002, the technology is available only in few centres.
Monochromatic Excimer Light (IPL) Therapy Other forms of targeted light therapy have been introduced, such as IPL therapy with wavelength of 304 nm (excilite: Deka) and 308 nm (Pxlite). These machines are less bulky, cheaper, and have a comparatively larger treatment surface in contrast to excimer laser. Several studies have been published which demonstrate their efficacy. In a pilot study of excimer light in 37 patients of vitiligo, Leone et al, [27] obtained initial repigmentation in the first 8 treatments and excellent repigmentation in 50% of patients at 6 months. Some patients who had not previously responded to narrowband UVB therapy were also found to respond. The results were comparable to excimer laser and superior to narrowband phototherapy. Another study demonstrated the efficacy of excimer light in a number of UV-responsive conditions such as palmoplantar psoriasis, atopic dermatitis, and alopecia areata. [28] IPL was also shown to induce apoptotic and immunohistochemical changes in psoriatic skin.[29] Thus excimer light is a promising, effective, and cheaper alternative to excimer laser.
Light-Based (Nonlaser, Non -IPL) Targeted Phototherapy
Advances in technology have now permitted delivery of conventional noncoherent light (broadband or narrowband light) targeted at lesions. Many such machines have been marketed in recent years (Sallman, Theralight, multilight, curelight, Bioskin, B-clear, etc). Most of these machines use a conventional high-pressure burner emitting UV light and fiber-optic cable systems to deliver energy directly targeted at the lesion. Their spot sizes range from 1 to 3 cm. These machines have multiple delivery programs and automatic calibration for quick delivery of predetermined dosages, so that treatment time is short. They are considerably smaller in size than the laser machines, with less maintenance problems, and are also cheaper. An added advantage of some of these machines over the excimer light or laser is that both UVA and UVB (narrowband) spectra are available. Several studies have been published on the efficacy of these systems in both vitiligo and psoriasis. [30],[31],[32],[33],[34],[35],[36]
Each of the different commercially available systems has its advantages and disadvantages, which are discussed below.
Dualight
(Previously called Theralight) emits both UVA radiation in the range 330-380 nm and UVB in the range 290-330 nm with peak at 303 nm 5 The system has a 2-meter long fiber-optic delivery system, with a spot size of 4 cm 2 . UVA intensity is 10-550 mW/cm² for 3.63-cm² exit aperture, while UVB intensity is 50-250 mW/cm² for 3.63-cm² exit aperture.
B clear targeted photoclearing system
B clear system is mercury-based noncoherent UVB radiation with a therapeutic wavelength of 290 to 320 nm and pulse width of 0.5 to 2.0 seconds. Fluence ranges from 50 to 800 mJ/cm 2 in increments of 10 mJ/cm 2 . Its disadvantage is that only UVB range is available, unlike Dualight, which delivers both UVA and UVB ranges. [30]
Bioskin
Lotti et al reported efficacy of a targeted narrowband UVB device in vitiligo in 1999. [31] Bioskin consisted of a mercury arc lamp with wavelength 280 to 320 nm and peak at 311 nm and a delivery system consisting of liquid-component optical fiber with spot size 1 cm in diameter. Seventy-five percent repigmentation was achieved in 5 of the 8 patients with segmental vitiligo, after 6 months′ treatment. A large study in 734 patients [32] showed 75% or more improvement in nearly 70% of the patients and total repigmentation in 21% of the subjects. No patient showed acute or chronic side effects.
Author′s experience
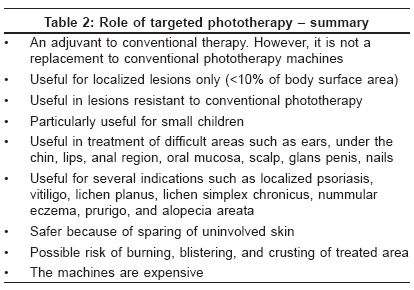
The author has used a targeted phototherapy device procured from the German company Salmann in 75 patients since 2003. This system is a lightweight, tabletop machine, with a weight of 9.3 kg, a fiber-optic delivery cable of length 2 meters, and spot size of 1 cm. It delivers UVA in the range 340-360 nm and UVB with a peak at 313 nm. It can deliver 100 mJ of UVB in 6 seconds. It does not have an automated delivery system as in B clear or Dualight machines and is therefore slower, but is also cheaper. In the author′s experience, targeted phototherapy is a very useful adjuvant to conventional phototherapy devices and provides many advantages [Table - 2]. Importantly, it is of a great value addition in dermatological practice and enables the clinician to treat many patients with resistant lesions and lesions in difficult areas, which are otherwise difficult to treat by conventional UVB machines. Another advantage is in treating children, who may feel intimidated by the large phototherapy machines. The machine is effective particularly in areas such as face, knee, trunk, eyelids, etc. but is not effective in UV-resistant areas such as fingertips. The biggest advantage is the ability to deliver energy without risk of acute or chronic side effects on unaffected skin. Thus patients, particularly those who have apprehensions about taking UV therapy, feel more comfortable with these machines. However, despite these advantages, they cannot replace the whole body machines and hand-foot machines, as large areas cannot be treated with targeted phototherapy. The higher cost of the machines is also an important consideration in the Indian situation.
Conclusion [Table - 2] summarizes the role of targeted phototherapy in current practice. As new data emerge, the role of this modality both in diseases such as vitiligo, [37] psoriasis [38],[39] and also in new indications such as acne [40] and stretch marks [41] continues to evolve. New technologies continue to emerge, such as new low-level helium neon laser system (reported to be effective in segmental vitiligo). [42] It is obvious that both targeted laser and nonlaser phototherapies represent exciting advances in dermatotherapy.
References
| 1. | Diffey BL. Ultraviolet phototherapy of skin diseases. Physics and Engineering in Medicine in the New Millennium, IPEM; 2000. p. 65-7. Back to cited text no. 1 |
| 2. | Bethea D, Fullmer B, Syed S, Seltzer G, Tiano J, Rischko C, et al. Psoralen photobiology and photochemotherapy: 50 years of science and medicine. J Dermatol Sci 1999;19:78-88 Back to cited text no. 2 |
| 3. | Hamzavi I, Lui H. Using light in dermatology: An update on lasers, ultraviolet phototherapy, and photodynamic therapy. Dermatol Clin 2005;23:199-207. Back to cited text no. 3 |
| 4. | Spencer JM, Hadi SM. The excimer lasers. J Drugs Dermatol 2004;3:522-5 Back to cited text no. 4 |
| 5. | Grimes PE. Advances in the treatment of vitiligo: Targeted phototherapy. Cosm Dermatol 2003;16:18-22 Back to cited text no. 5 |
| 6. | Spencer JM, Nossa R, Ajmeri J. Treatment of vitiligo with the 308-nm excimer laser: A pilot study. J Am Acad Dermatol 2002;46:727-31. Back to cited text no. 6 |
| 7. | Young AR, Chadwick CA, Harrison GL, Nikaido O, Ramsden J, Potten CS. The similarity of action spectra for thymidine dimmers in human epidermis and erythema suggests that DNA is the chromophore for erythema J Invest Dermatol 1998;111:982-8 Back to cited text no. 7 |
| 8. | Cooper KD. Cell mediated immunosuppressive mechanisms induced by UV radiation photochemistry and photobiology. Photochem Photobiol 1996;63:400-5 Back to cited text no. 8 |
| 9. | Yaron I Yaron R, Oluwole SF, Hardy MA. UVB radiation of human derived peripheral blood lymphocytes induces apoptosis but not T cell anergy. Cell immunol 1996;168:258-66 Back to cited text no. 9 |
| 10. | Freeman SE, Gange RW, Sutherland JC, Matzinger EA, Sutherland BM. Production of pyrimidine dimmers in DNA of human skin exposed in situ to UVA radiation. J Invest Dermatol 1987;88:430-3. Back to cited text no. 10 |
| 11. | Taneja A, Trehan M, Taylor CR. 308-nm excimer laser for the treatment of localized vitiligo. Int J Dermatol 2003;42:658-62. Back to cited text no. 11 |
| 12. | Asawanonda P, Anderson RR, Chang Y, Taylor CR. 308-nm excimer laser for the treatment of psoriasis: A dose-response study Arch Dermatol 2000;136:619-24. Back to cited text no. 12 |
| 13. | Morison WL, Atkinson DF, Werthman L. Effective treatment of scalp psoriasis using the excimer (308 nm) laser Photodermatol. Photoimmunol Photomed 2006;22:181-3 Back to cited text no. 13 |
| 14. | Rodewald EJ, Housman TS, Mellen BG, Feldman SR Follow-up survey of 308-nm laser treatment of psoriasis. Lasers Surg Med 2002;31:202-6. Back to cited text no. 14 |
| 15. | Kollner K, Wimmershoff M, Landthaler M, Hohenleutner U. Treatment of oral lichen planus with the 308-nm UVB excimer laser-early preliminary results in eight patients. Lasers Surg Med 2003;33:158-60 Back to cited text no. 15 |
| 16. | Gundogan C, Greve B, Raulin C. Treatment of alopecia areata with the 308-nm xenon chloride excimer laser: Case report of two successful treatments with the excimer laser. Lasers Surg Med 2003;33:158-60. Back to cited text no. 16 |
| 17. | Baltas E, Csoma Z, Bodai L, Ignacz F, Dobozy A, Kemeny L. Treatment of atopic dermatitis with the xenon chloride excimer laser. J Eur Acad Dermatol Venereol 2006;20:657-60. Back to cited text no. 17 |
| 18. | Kontos AP, Kerr HA, Malick F, Fivenson DP, Lim HW, Wong HK. 308-nm Excimer laser for the treatment of lymphomatoid papulosis and stage IA mycosis fungoides Photodermatol Photoimmunol Photomed 2006;22:168-71 Back to cited text no. 18 |
| 19. | Goldberg DJ, Sarradet D, Hussain M. 308-nm Excimer laser treatment of mature hypopigmented striae. Dermatol Surg 2003;29:596-8 Back to cited text no. 19 |
| 20. | Goldberg DJ, Marmur ES, Schmults C, Hussain M, Phelps R. Histologic and ultrastructural analysis of ultraviolet B laser and light source treatment of leukoderma in striae distensae. Dermatol Surg 2005;31:385-7. Back to cited text no. 20 |
| 21. | Alexiades-Armenakas MR, Bernstein LJ, Friedman PM, Geronemus RG. The safety and efficacy of the 308-nm excimer laser for pigment correction of hypopigmented scars and striae alba. Arch Dermatol 2004;140:955-60. Back to cited text no. 21 |
| 22. | Kφllner K, Wimmershoff MB, Hintz C, Landthaler M, Hohenleutner U. Comparison of the 308-nm excimer laser and a 308-nm excimer lamp with 311-nm narrowband ultraviolet B in the treatment of psoriasis. Br J Dermatol 2005;152:750-4. Back to cited text no. 22 |
| 23. | Rivort J. Experience with excimer laser. J Drugs Dermatol 2006;5:550-4 Back to cited text no. 23 |
| 24. | Choi KH, Park JH, Ro YS. Treatment of Vitiligo with 308-nm xenon-chloride excimer laser: Therapeutic efficacy of different initial doses according to treatment areas. J Dermatol 2004;31:284-92 Back to cited text no. 24 |
| 25. | Passeron T, Ostovari N, Zakaria W, Fontas E, Larrouy JC, Lacour JP, et al . Topical tacrolimus and the 308-nm excimer laser: A synergistic combination for the treatment of vitiligo Arch Dermatol 2004;140:1065-9. Back to cited text no. 25 |
| 26. | Ferguson J. The 308-nm excimer laser is practical therapy for psoriasis. J Watch Dermatol January 14, 2003. Back to cited text no. 26 |
| 27. | Leone G, Iacovelli P, Paro Vidolin A, Picardo M. Monochromatic excimer light 308 nm in the treatment of vitiligo: A pilot study. J Eur Acad Dermatol Venereol 2003;17:531-7 Back to cited text no. 27 |
| 28. | Aubin F, Vigan M, Puzenat E, Blanc D, Drobacheff C, Deprez P, et al . Evaluation of a novel 308-nm monochromatic excimer light delivery system in dermatology: A pilot study in different chronic localized dermatoses. Br J Dermatol 2005;152:99-103. Back to cited text no. 28 |
| 29. | Bianchi B, Campolmi P, Mavilia L, Danesi A, Rossi R, Cappugi P. Monochromatic excimer light (308 nm): An immunohistochemical study of cutaneous T cells and apoptosis-related molecules in psoriasis. J Eur Acad Dermatol Venereol 2003;17:408-13. Back to cited text no. 29 |
| 30. | Gilles PR. Technical evaluation of fibre optically delivered light for lesion targeted high dosage UVB phototherapy B-clear application note 2 Lumenis inhouse publication 2002 Back to cited text no. 30 |
| 31. | Lotti TM, Menchini G, Andreassi L. UV-B radiation microphototherapy: An elective treatment for segmental vitiligo. J Eur Acad Dermatol Venereol 1999;13:102-8. Back to cited text no. 31 |
| 32. | Menchini G, Tsoureli-Nikita E, Hercogova J. Narrow-band UV-B micro-phototherapy: A new treatment for vitiligo. J Eur Acad Dermatol Venereol 2003;17:171-7 Back to cited text no. 32 |
| 33. | Kaur M, Oliver B, Hu J, Feldman SR. Nonlaser UVB-targeted phototherapy treatment of psoriasis. Cutis 2006;78:200-3. Back to cited text no. 33 |
| 34. | Toll A, Vιlez-Gonzαlez M, Gallardo F, Gilaberte M, Pujol RM. Treatment of localized persistent plaque psoriasis with incoherent narrowband ultraviolet B phototherapy. J Dermatol Treat 2005;16:165-8. Back to cited text no. 34 |
| 35. | Asawanonda P, Charoenlap M, Korkij W. Treatment of localized vitiligo with targeted broadband UVB phototherapy: A pilot study. Photodermatol Photoimmunol Photomed 2006;22:133-6 Back to cited text no. 35 |
| 36. | Amornpinyokeit N, Asawanonda P. 8-methoxypsoralen cream plus targeted narrowband ultraviolet B for psoriasis Photodermatol Photoimmunol Photomed 2006;22:285-9 Back to cited text no. 36 |
| 37. | Hadi S, Tinio P, Al-Ghaithi K, Al-Qari H, Al-Helalat M, Lebwohl M, et al Treatment of vitiligo using the 308-nm excimer laser. Photomed Laser Surg 2006;24:354-7 Back to cited text no. 37 |
| 38. | He YL, Zhang XY, Dong J, Xu JZ, Wang J. Clinical efficacy of a 308 nm excimer laser for treatment of psoriasis vulgaris. Photodermatol Photoimmunol Photomed 2007;23:238-41 Back to cited text no. 38 |
| 39. | Lapidoth M, Adatto M, David M. Targeted UVB phototherapy for psoriasis: a preliminary study. Clin Exp Dermatol 2007;32:642-5 Back to cited text no. 39 |
| 40. | Noborio R, Nishida E, Kurokawa M, Morita A. A new targeted blue light phototherapy for the treatment of acne. Photodermatol Photoimmunol Photomed 2007;23:32-4. Back to cited text no. 40 |
| 41. | Sadick NS, Magro C, Hoenig A. Prospective clinical and histological study to evaluate the efficacy and safety of a targeted high-intensity narrow band UVB/UVA1 therapy for striae alba. J Cosmet Laser Ther 2007;9:79-83 Back to cited text no. 41 |
| 42. | Yu HS, Wu CS, Yu CL, Kao YH, Chiou MH. Helium Neon laser irradiation stimulates migration and proliferation in melanocytes and induces repigmentation in segmental vitiligo. J Invest Dermatol 2003;120:56-64. Back to cited text no. 42 |
Copyright 2009 - Indian Journal of Dermatology, Venereology and Leprology
The following images related to this document are available:
Photo images
[dv09038t2.jpg]
[dv09038t1.jpg]
|

{kind=link}
{kind=link}