 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
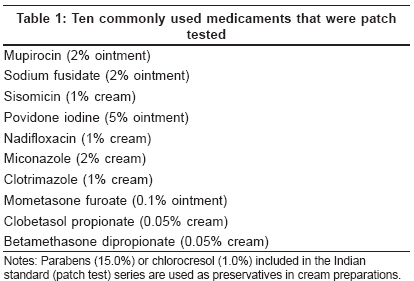
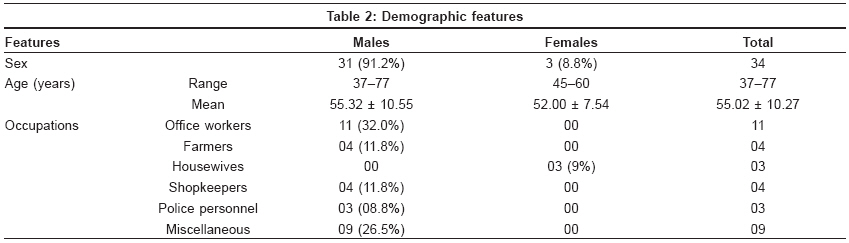
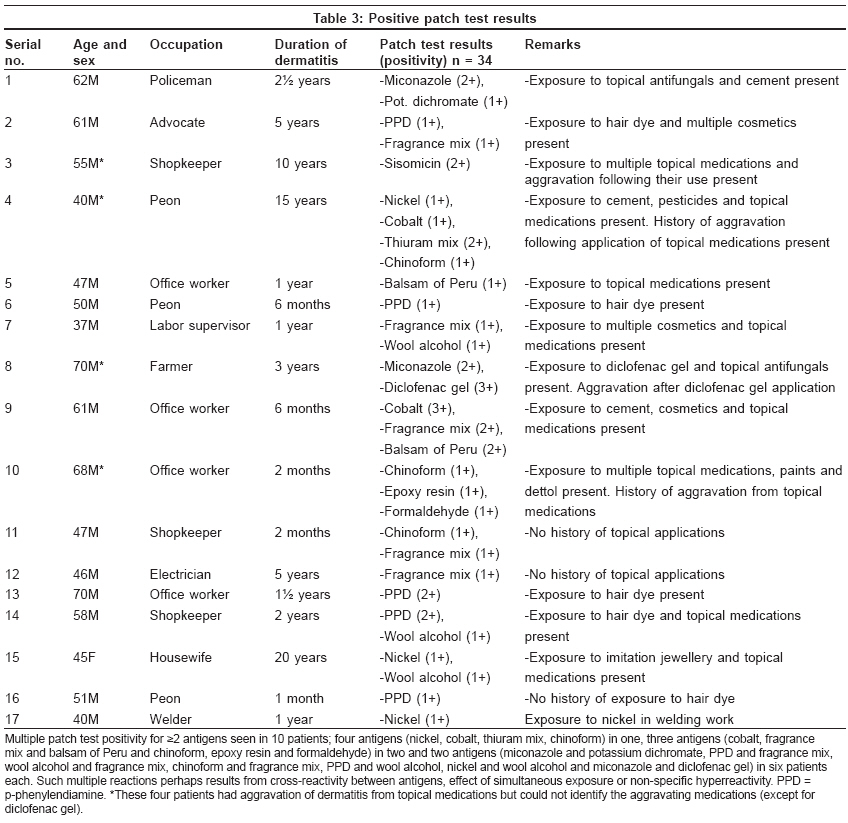
Indian Journal of Dermatology, Venereology and Leprology, Vol. 75, No. 2, March-April, 2009, pp. 136-141 Original Article Contact sensitization in venous eczema: Preliminary results of patch testing with Indian standard series and topical medicaments Jindal Rashmi, Sharma Nand Lal, Mahajan Vikram K, Tegta Gita Ram Department of Dermatology, Venereology and Leprosy, Indira Gandhi Medical College, Shimla Code Number: dv09040 Abstract Background and Aims: Elimination of allergens/topical medications causing contact dermatitis in venous eczema, which poses a significant problem in its chronicity and treatment, provides the basis for better therapeutic outcome. Our objective was to determine the pattern of contact sensitization in venous eczema patients in Himachal Pradesh (India). Methods: Thirty-four patients (M:F, 31:3) and 10 controls (M:F, 6:4) were patch tested with Indian standard series and 10 commonly used topical medicaments.Results: Positive patch test results were seen in 50% (M:F, 16:1) of the patients. Common allergens were Fragrance mix (15%), p-phenylendiamine (15%), nickel (9%), wool alcohol (9%), chinoform (9%), balsum of Peru (5%), cobalt chloride (5%), potassium dichromate (3%), epoxy resin (3%), thiuram mix (3%) and formaldehyde (3%). Only sisomycin and miconazole among the topical medications elicited a positive patch test reaction in 3 and 5% patients, respectively. Neomycin contact sensitivity was not seen in any of the patients. One patient who had exacerbation of venous eczema following accidental application of topical diclofenac showed a positive patch test reaction to it. Conclusions: Patch test should be used to identify the topical agents that may be responsible for perpetuation or aggravation of eczema, especially in patients who do not improve despite adequate treatment of other underlying cause(s). Keywords: Dermatitis medicamentosa, gravitational eczema, miconazole, patch testing, sisomycin, stasis dermatitis Introduction Venous eczema (synonyms: stasis dermatitis, gravitational eczema) secondary to venous hypertension is a common condition that usually presents as eczematous lesions around the ankles and lower legs. Varicose veins are commonly associated with patches of dermatitis arising preferentially over them. The condition is intensely pruritic and other features of venous hypertension like leg edema (more towards evening), hemosiderin depositions, venous ulcerations, small patches of atrophic telangiectatic scarring and lipodermatosclerosis develop over a period. These changes often get modified by secondary contact dermatitis, scratching and infection. Allergic contact dermatitis due to topically applied medicaments is a common complication of venous eczema, with an estimated incidence of contact sensitization as high as 40-90%. [1] Dissemination of dermatitis may occur to face or hands, occasionally progressing to erythroderma. Patches of eczema may also develop on the other leg even when it is not affected by obvious venous insufficiency due to dissemination or secondary sensitization from medications applied on the affected leg. Contact sensitization needs to be suspected in patients showing resistance to apparently adequate therapy and in those who complain of intolerance to a particular topical treatment. Early recognition and treatment of allergic contact dermatitis in these patients is imperative for better therapeutic outcome. Commonly used medicaments that may act as a sensitizer are usually included in standard patch test batteries. However, results of patch testing vary across regions and, at a given time, depend on the local prescribing habits and topical medications in vogue. Moreover, these patients habitually apply, whether prescribed or not, a wide range of medicaments that may have a sensitizing potential. In this study, we present patch test results for Indian standard series and topical medicaments in venous eczema patients. Methods Thirty-four consecutive patients (excluding pregnant/lactating females) of venous eczema attending the Outpatient Dermatology Department of Indira Gandhi Medical College, Shimla, were patch tested during July 2005-June 2006. Institute ethical committee cleared the project. Patients having acute dermatitis were tested after the acute episode subsided or when the dose of prednisolone was < 20 mg/day. Clinical details regarding age, sex, occupation, duration and progress of dermatitis, aggravating factors, treatment taken and atopy were recorded. Special attention was given to the nature of the topical medications used. A thorough clinical examination and charting of lesions was performed. Ten subjects were also selected as controls from patients having minor dermatoses other than dermatitis. After obtaining written consent, the patch test antigens comprising 10 commercially available and commonly used topical medicaments [Table - 1] along with Indian standard (patch test) series (purchased from Systopic India Ltd., New Delhi, India) [2] were patch tested by the Finn Chamber method. Finn Chambers were applied on the upper back and the patients returned for determination of results after both days 2 and 3. Results were graded as per the International Contact Dermatitis Research Group criteria. [3] Results The demographic features of these 34 patients (M:F, 31:3) are shown in [Table - 2]. They were between 37 and 77 (mean 55.02 ± 10.27) years of age. Twenty (59%) patients were aged between 51 and 70 years and comprised the majority. Eleven (32%) patients were office workers doing sedentary work for 6-8 h every day. All three females were engaged in housework; two of them were also involved in farming. The duration of dermatitis varied from 1 month to 20 years (mean 43.7 months) and 28 (82.4%) patients had presented within 5 years of developing dermatitis. Ten (29%) patients with long-standing disease reported episodes of relapses and remissions. Five (15%) patients had aggravation of dermatitis on prolonged standing. Four (12%) patients correlated aggravation of dermatitis to application of various topical medications; however, they could not name/identify these specifically. One patient (3%) developed acute exacerbation of dermatitis following accidental application of topical diclofenac gel prescribed for joint pains. The remaining patients could not attribute aggravation of dermatitis to any specific topical medication that they had been using. Patch test results were positive in 17 (50%) (M:F, 16:1) patients [Table - 3]. Fragrance mix and p -phenylendiamine (PPD) were the most common allergens in five (15%) patients each. Nickel sulfate, wool alcohols and chinoform showed sensitivity in three (9%) patients each. Two (5%) patients each showed a positive reaction to balsam of Peru or cobalt chloride. Sensitivity to potassium dichromate, epoxy resin, thiuram mix or formaldehyde was observed in one (3%) patient each. Among the topical medications tested, sensitivity to sisomicin was observed in one (3%) and miconazole in two (5%) patients, respectively. None of the other topical medications elicited a positive reaction. Ten (29%) patients showed sensitivity to ≥2 allergens [Table - 3]. One patient had sensitivity to a maximum of four patch test antigens (nickel, cobalt, thiuram mix, chinoform). The patient having aggravation of dermatitis following topical application of diclofenac gel showed a 3+ reaction. Ten controls (M:F, 6:4) aged between 26 and 64 years were involved in various occupations, such as farming, clerical jobs and household work. Only one subject, a 32-year-old male, showed a positive reaction to PPD. Discussion Venous eczema usually affects the elderly or middle-aged individuals, without any predilection for gender. However, females are affected more often, presumably due to hormonal effects or increased intra-abdominal pressure and tendency for deep vein thrombosis during pregnancy. The risk of developing stasis dermatitis increases with each passing decade owing to the presence of chronic skin disorders like stasis eczema, asteatotic eczema and leg ulcers requiring long-term topical therapy that may cause contact sensitivity, and its reported prevalence in adults older than 70 years exceeds 20%. [4],[5],[6] Prolonged standing is another risk factor for developing venous insufficiency/venous eczema or its chronicity. [7] Most of our patients comprised office workers (32%), shopkeepers (12%), farmers (12%), peons (9%) and policemen (9%), professions which involved long hours of standing or sitting with their legs in a dependent position, and 59% were in the age group of 51-70 years. Allergy to components of topical preparations is common in patients of chronic dermatitis and leg ulcers that often complicates and prolongs the treatment. The reported prevalence of contact sensitivity in these patients is 57.8-71.5%. [1],[8],[9],[10] This higher incidence may be due to selection of patients during exacerbations or when the dermatitis is not responding to treatment. The real incidence of contact dermatitis in stasis dermatitis perhaps lies between 50 and 60% if all patients of venous eczema are patch tested. [1] Fifty percent of our patients showed patch test positivity to one or more antigens. Angelini et al. [8] reported contact sensitivity to PPD in 16% of their venous eczema patients, which seems comparable to that of 15% in our patients. PPD is present in hair and fur dyes, photographic developers, oils, greases, gasoline and rubber/plastic. It cross-reacts commonly with para amino compounds and p -amino benzoic acid. According to Fraki et al , [11] the PPD sensitivity is quite uncommon. However, according to Breit, [1] the incidence of PPD sensitivity in venous eczema patients has remained steady over time. This probably reflects differences in the use of these compounds across countries. In daily life, PPD comes in contact easily due to its use in dyes used for socks, trousers, shoes and hair colorants, leading to positive patch test reactions in a fair proportion of healthy subjects. Patch test positivity to PPD in our five patients and one control without any cross reactivity to the parabens, the common preservative in topical preparations, can apparently be attributed to the use of hair dye or articles of daily use. Another common sensitizer in our study was fragrance mix, eliciting positive patch test reactions in 14% of the patients. It is a mixture of cinnamic aldehyde, cinnamic alcohol, hydroxycitronellal, amylcinnamaldehyde, geraniol, eugenol, isoeugenol and oakmoss absolute in 1% concentration each. Exposure is commonly through cosmetics and toiletries, food items and other household products. The incidence of contact sensitization with fragrance mix in patients with chronic venous insufficiency is about 8.3%, perhaps as a result of frequently used fragrance-containing emollients. [12] This can also be corroborated from the fact that three of our five patients with fragrance mix sensitivity had been using various over-the-counter creams/lotions. Wool alcohol and balsam of Peru are commonly associated with contact sensitivity. The reported incidence in various studies is 21-33% for wool alcohols and 19-23% for balsam of Peru, respectively.[11],[12],[13] Our figures of 9 and 5% are comparable to those of Angelini et al , [8] who observed an incidence of 8.9 and 4.5% respectively for contact sensitivity to wool alcohol and balsam of Peru. Wool alcohol is used in cosmetics and pharmaceuticals, furniture polish, paper, leather, inks, textiles, oil emulsions and waxes while balsam of Peru is a common constituent of perfumes, topical medicaments and flavors for edibles. Almost all our patients had a history of frequent use of various topical medicaments over a period of time and might have developed contact sensitization to them. Chinoform (iodochlorhydroxyquin), a weak and infrequent sensitizer, is used as an anti-infective and anti-amoebic agent for topical or systemic use. Cross-reactions with other halogenated hydroxyquinilones may occur. [14] Breit and Bandmann [15] observed chinoform sensitivity in their 3.1% patients of stasis ulcers and eczema. Although we observed chinoform sensitivity in 9% of our patients, they also had simultaneous sensitivity to nickel, cobalt, thiuram mix, fragrance mix, epoxy resin and formaldehyde for unexplained reasons. Similar observations were also made by Cronin. [16] Sensitization to metals like potassium dichromate, nickel sulfate and cobalt chloride from day to day exposure is frequent. Nickel had been the most notorious sensitizer in the past, perhaps due to its widespread use in imitation jewellery, watches, buttons, zippers, rings, doorknobs, batteries, metal-cutting fluids, coins, orthopedic plates, keys, spectacle frames and kitchenware. Similarly, cobalt chloride is a component of paints, jewellery, zippers, buttons, utensils, hair dyes and cosmetics while potassium dichromate finds use in cement, leather tanning, textile dyes, wood preservatives, photography, welding, shoe polishes, paints, detergents, electroplating and automobile industry. Various studies report sensitivity to potassium dichromate (4.0-13.9%), nickel (2.3-16.7%) and cobalt (1.3-5.6%) in venous eczema patients. [8],[12] In our study, 3, 9 and 5% of the patients reacted to potassium dichromate, nickel and cobalt respectively and were sensitized probably from articles of daily use. Nickel sensitivity in one female patient could be correlated to the use of trinkets. Patients sensitive to potassium dichromate and cobalt were engaged in masonry while another patient sensitive to thiuram mix was a spare time agriculturist, the occupations well known to predispose for sensitization by these allergens. Formaldehyde is used in the production of urea, phenolic melamine and acetate resin. It also finds use as an astringent, disinfectant and preservative in cosmetics, shampoos and metal-working fluids. It is also commonly detected in tubes containing topical medications as a result of degradation of synthetic resins in the inner coating of tubes and has been reported to be associated with contact sensitization in 0.67-4.2% of the cases. [8],[11] Probably for a similar reason, only one (3%) of our patients showed positive patch test reactions to formaldehyde. Thiuram mix finds use as an accelerator and activator for natural rubber, bacteriostatic, animal repellent, seed disinfectant and fungicide. Exposure to epoxy resins occurs from their use in adhesives, surface coatings, plasticizers, paints, inks, etc. In our study, one (3%) patient engaged in farming showed a positive patch test to thiuram mix and another to epoxy resin, probably from occupational exposure to them. Of the topical medications tested, positive reactions were obtained due to sisomicin in one (3%) and miconazole in two (5%) patients, respectively. Marquis et al , [17] in their multicenter study, observed only 0.64% of test sites having weak positive reaction for sisomycin after 4 days of application while Saha et al, [18] noted contact sensitivity to sisomicin in their 16% patients of footwear dermatitis. Its low sensitization potential was evident in our study despite its widespread use lately. Among the antimycotics, allergic contact dermatitis to miconazole and clotrimazole has been reported by Raulinc and Frosch. [19] Five percent of our patients showed positive patch test reactions to miconazole, who had been sensitized probably from its frequent use by them. It will be pertinent to mention here that none of our patients was found sensitive to neomycin, a frequent sensitizer until few years back. Angelini et al , [8] in their two separate studies of 1968-1977 and 1978-1983, respectively, observed neomycin sensitivity declining from 7.3 to 3.1%. Similarly, in the 1980s, Pasricha et al [20] and Bajaj et al, [21] from India reported neomycin sensitivity in 28 and 48%, respectively. This has declined further (7% of 1003 patch-tested patients) in a recent study of 2007 by Bajaj et al. [22] This overall decreasing incidence of neomycin sensitivity is perhaps due to its infrequent use now a days due to its well-recognized sensitizing potential. Contact sensitization to active drugs or to their constituents is a continuously operating factor and is one of the factors responsible for the chronicity and deterioration in stasis dermatitis. Patch test should be used to identify the topical agents that may be responsible for perpetuation or aggravation of eczema, especially in patients who do not improve despite adequate treatment of other underlying cause(s). Additionally, it is imperative to consider unprescribed medications causing sudden exacerbation of existing dermatitis. The significance of patch testing with these need to be emphasized, especially in patients such as the one who developed exacerbation of venous eczema following accidental application of topical diclofenac. References
Copyright 2009 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv09040t3.jpg] [dv09040t1.jpg] [dv09040t2.jpg] |
| |||||||||


{kind=link}
{kind=link}
{kind=link}