 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
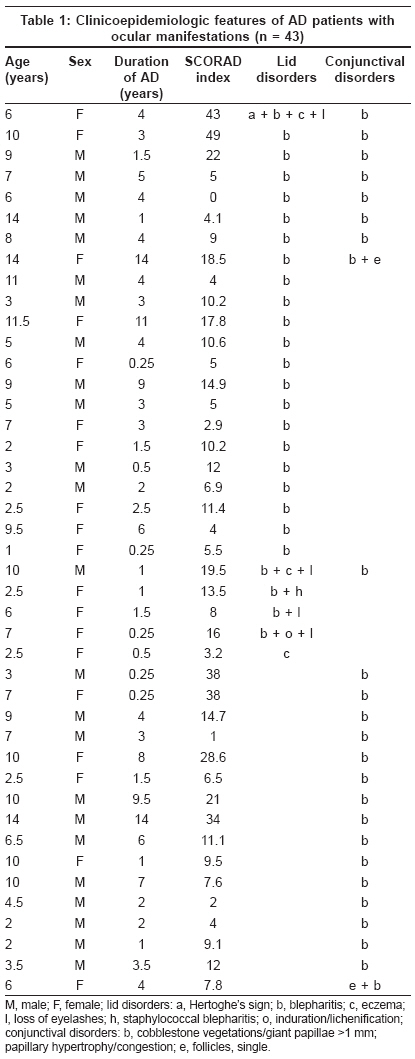
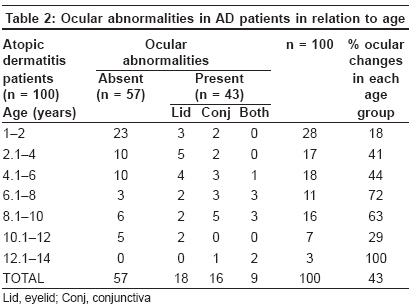
Indian Journal of Dermatology, Venereology and Leprology, Vol. 75, No. 2, March-April, 2009, pp. 148-151 Original Article Ocular abnormalities in atopic dermatitis in Indian patients Kaujalgi Radhika, Handa Sanjeev, Jain Arun, Kanwar AmrinderJ Department of Dermatology, Venereology and Leprology, Postgraduate Institute of Medical Education and Research, Chandigarh Code Number: dv09042 Abstract Background and Aims: Atopic dermatitis (AD) is a common skin disease. Long-standing, severe AD with repeated scratching and rubbing of the face, which requires continuous dermatologic care, predisposes the patient to various ocular complications. The knowledge of the frequency and significance of these ocular complications may allow their early diagnosis and treatment. The present study assesses the ocular complications in Indian children suffering from AD.Methods: In order to study the ocular complications in AD, 100 patients (61 male and 39 female) between the ages of 1 and 14 years were recruited. All the patients had complete dilated fundus examination with indirect ophthalmoscopy. The lid, conjunctiva and cornea were examined. Also, any evidence of cataract formation and retinal disorders were recorded. Results: The mean age of the children was 5.4 years. Forty-three (43.0%) AD patients showed ocular abnormalities in the form of lid and conjunctival changes. Of these, 18 (41.9%) patients showed only lid involvement, 16 (37.2%) only conjunctival involvement and both conjunctival and lid changes were seen in nine (20.9%) patients. Conjunctival changes were mostly in the form of a cobblestone appearance of the papillae, with mild to moderate papillary reaction and papillary hypertrophy. Variables observed to have a significant impact on the development of ocular abnormalities were age more than 5 years, duration of illness >12 months, positive family history of atopy, presence of palmar hyperlinearity and a combination of both xerosis and Dennie-Morgan fold. Conclusions: The present study is the first of its kind from India to document an association between AD in children and various ocular manifestations. The ocular manifestations observed in our cohort were not associated with significant ocular morbidity or visual impairment possibly because of a less-severe disease in Indians. Keywords: Atopic dermatitis, children, ocular abnormalities Introduction Atopic dermatitis (AD) is a pruritic, chronic, relapsing inflammatory disease of the skin that affects genetically predisposed individuals and may express itself either as the infantile, childhood or adult eczema, with changing morphology and localization. [1] The disease activity is often characterized by remissions and recurrences. Long - standing, severe AD with repeated scratching and rubbing of the face, which requires continuous dermatologic care, predisposes the patient to various ocular complications. The complications may include dermatitis of the eyelids, [2] blepharitis, [2] keratoconjunctivitis, keratoconus, [3],[4],[5] uveitis, [4],[5],[6] anterior and posterior subcapsular cataract, [5],[6],[7] retinal detachment [8] and ocular herpes simplex. [2],[3],[4],[5],[6],[7],[8],[9],[10] The knowledge of the frequency and significance of these ocular complications may allow their early diagnosis and treatment. The present study assesses the ocular complications in Indian children (up to 14 years of age) suffering from AD. This, to the best of our knowledge, is the first study of its kind from this part of the world. Methods One hundred consecutive patients with AD attending the Pediatric Dermatology Clinic at our center, a tertiary care referral center, were taken up for the study and institute ethics committee approved the project. Diagnosis of AD in each patient was made according to the Williams (U.K. Working party) diagnostic criteria.[11] Detailed demographic parameters, including symptoms, total disease duration, personal or family history of other atopic diseases, treatment history in the form of topical steroids, antihistamines, emollients, etc. were recorded in the clinic proforma. Children on systemic corticosteroid therapy were excluded from the study. All the patients had complete dilated fundus examination with indirect ophthalmoscopy. The lid, conjunctiva and cornea were examined. Also, any evidence of cataract formation and retinal disorders was recorded. The severity and extent of AD was evaluated using a SCORAD index [12] at the time of evaluation of the patient. Based on this, the patients were classified into the following three categories: mild disease (SCORAD < 20), moderate disease (SCORAD 20.1-40) and severe disease (SCORAD > 40). The relationship between the ocular findings and the clinical severity of AD (as assessed using the SCORAD index) was determined. χ2 test was used for the statistical analysis of the various parameters in relation to ocular abnormalities. Informed consent was taken from the patient′s guardians before the start of the study. Results Of the 100 children, 61 were male and 39 were female. The male to female ratio was 1.56:1. The mean age of the children was 5.4 years (SD ± 3.76), range being 1-14 years. Forty-three (43%) AD patients showed ocular abnormalities in the form of lid and conjunctival changes. Of these, 18 (41.9%) patients showed only lid involvement, 16 (37.2%) only conjunctival involvement and both conjunctival and lid changes were seen in nine (20.9%) patients. Among the 18 patients with lid involvement, 16 had isolated blepharitis and the remaining two had loss of the eyelashes and eczema of the eyelids along with blepharitis [Table - 1]. Conjunctival changes in the form of papillae or cobblestone appearance of the papillae, with mild to moderate papillary reaction and papillary hypertrophy was noted in 15 patients. Sixteen of the 52 children less than 5 years of age had ocular abnormalities while 27 of the 48 children more than 5 years of age had ocular abnormalities. This was statistically significant ( P -value = 0.010). Among the 43 AD patients with ocular changes, maximum eye changes were seen in 10 (23.2%) patients in the age group of 8.1-10 years. Maximum lid abnormalities were seen in five (11.6%) patients in the age group of 2.1-4 years, whereas maximal involvement of the conjunctiva was noticed in five (11.6%) patients in the age group of 8.1-10 years. This difference was statistically insignificant ( P -value = 0.300) [Table - 2]. The mean SCORAD index in 43 patients with ocular abnormalities was 13.39 (SD + 11.77) whereas it was 14.94 (SD + 11.77) in AD patients with no ocular abnormalities. This difference was statistically insignificant ( P -value = 0.932). Our patients did not have severe disease. Only four children during the study period had been put on corticosteroids and hence were not included in the study. There was no significant correlation between the presence of AD lesions over the face and ocular manifestations. A statistically significant difference ( P -value = 0.002) was seen in patients with disease duration> 12 months and development of ocular abnormalities. Among AD patients with ocular abnormalities, 19 (44.0%) had a positive family history of atopy. Of the 57 AD patients without ocular abnormalities, only 14 (24.6%) had a positive family history of atopy. The difference was statistically significant ( P -value = 0.039). However, no statistically significant difference was found in patients with positive personal history of atopy in the two groups. Of the 43 AD patients with ocular abnormalities, palmar hyperlinearity was present in nine (21.0%) whereas it was noted in only four (7.0%) of the 57 patients without ocular abnormalities. The difference was statistically significant ( P -value = 0.041). Twenty-one (49.0%) of the 43 patients had a combination of dryness of skin and Dennie-Morgan fold whereas only 14 (24.5%) of the 57 without ocular abnormalities had this combination of minor criteria. This difference was statistically significant ( P -value = 0.006). Discussion AD is an itchy, chronic, fluctuating inflammatory disease, with frequency varying from 0.7 to 26.0% [13] in different countries. Repeated rubbing and scratching of the face can lead to certain ocular manifestations, like periorbital darkening, [14] Hertoghe′s sign [10] and Dennie-Morgan fold. [15] The incidence of ocular complications in various studies conducted in different age groups has varied from 25 to 40%. [9],[10],[14],[15],[16] Of the 100 AD patients, only 43 (43%) had eye involvement. We found ocular involvement to be more common in males, unlike in other studies. [1],[6] Eye findings were limited to only the lid and conjunctiva and no other structure of the eye was affected in any of the patients. In earlier studies, eyelid changes have been reported to occur in 16-62.2% of the AD patients. [6],[17] Forty-two percent of our patients had only lid changes while only conjunctival changes were found in 37%, a figure higher than 16% mentioned by Garrity and Liesegang.[6] Keratoconus in AD patients has been observed in 0.5-39.0%. [18],[19] However, none of our patients had keratoconus. Garrity and Liesegang [6] found cataract and retinal detachment respectively in 13.0 and 7.5% of their 200 patients having severe disease and where the disease duration was as long as 29 years. Uehara et al. [20] observed cataract in 19 (12.4%) of the 153 AD patients between the ages of 12 and 30. Because in AD patients cataract or opacification of the lens is described in the second or third decades of life in patients with widespread skin disease. This complication was not expected in our cohort of patients with a mean age of only 5.4 years. The earlier studies have not used an objective measure like the SCORAD index for determining the exact severity of the disease. Serious ocular changes were probably not seen in our patients because the majority had a low SCORAD index. The mean duration of the disease in our patients with ocular changes was 3.6 years and 1.9 years in those without ocular changes. When arbitrarily classifying the disease duration as less than or more than 1 year, ocular changes were significantly more in AD patients with disease duration of more than 1 year ( P -value = 0.002). We found a statistically significant correlation between minor criteria of AD like palmar hyperlinearity and combination of xerosis and Dennie-Morgan fold and the presence of ocular changes. The significance of this correlation is subject to debate. [21],[22] Family history of atopy may be an important predictor for the development of eye changes because a positive family history of atopy was obtained in 19 (44%) of the 43 patients with ocular abnormalities and only 14 (25%) of the 57 patients without ocular abnormalities ( P -value = 0.039). Some workers have suggested a possible relationship between the development of ocular changes and a personal history of respiratory atopy. [20] This observation was not found to be significant in our study. Taniguchi et al. [23] showed a significant relationship between severe facial involvement and ocular changes. However, we found no significant correlation between facial involvement and ocular changes because the habitual rubbing of the face to relieve itching was minimal in our patients. In conclusion, the present study is the first of its kind from India to document an association between AD in children and various ocular manifestations. The ocular manifestations observed in our cohort were not associated with significant ocular morbidity or visual impairment possibly because of a less-severe disease in Indians. However, more long-term studies would help to confirm our findings. References
Copyright 2009 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv09042t2.jpg] [dv09042t1.jpg] |
| |||||||||

{kind=link}
{kind=link}