 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
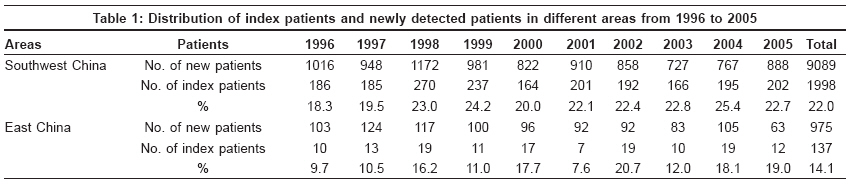
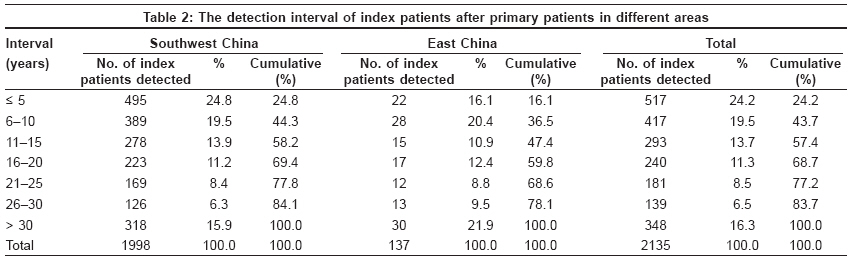
Indian Journal of Dermatology, Venereology and Leprology, Vol. 75, No. 2, March-April, 2009, pp. 152-156 Original Article Analysis on value of household contact survey in case detection of leprosy at a low endemic situation in China Shen Jianping, Wang Yaofei, Zhou Min, Li Wenzhong Department of Leprosy Control, Institute of Dermatology, Chinese Academy of Medical Sciences, Nanjing, PR, 210042 Code Number: dv09043 Abstract Background: Leprosy is at a low endemic situation in China, the value of house contact survey in case detection of leprosy becoming a dispute.Aims: To evaluate the value of household contact survey in the case detection of leprosy at a low endemic situation in China. Methods: A study was carried out using a designed questionnaire in a retrospective method to analyze the value of household contact survey in case detection in Southwest and East China. Results: A total of 2135 index leprosy patients were collected from January 1, 1996 to December 31, 2005 in six provinces of China. The number of index patients accounted for 22.0 and 14.1% of newly registered patients in the Southwest and East of China, respectively. The household contact survey (36.1%) and the skin clinic (62.0%) ranked first in methods of case detection in Southwest and East China, respectively. Within 5 years after primary leprosy patients were detected, 24.8 and 16.1% of the index patients in Southwest China and East China had been detected, respectively. Conclusion: The authors conclude that at the time of a low leprosy endemic situation, the household contact survey is still a useful method for case detection in China. Keywords: Case detection, household contacts, leprosy Introduction Transmission of leprosy within households is an old topic of the study in leprosy control for many years. However, what is its value of the household contact survey in China? Should we still insist on the household contact survey in case finding activity today? It had been reported [1] that household contact examination detected very few new patients within 5-10 years follow-up at a low endemic situation in East China′s Shandong province. In order to understand the value of the leprosy household contact survey in China, we carried out a special survey on leprosy household patients in three provinces in each Southwest and East China in 2006.Methods According to the annual report of leprosy data by each province at the end of 2005, three provinces, namely Yunnan, Sichuan and Guizhou Province, with a relative high case detection rate of 0.303-0.91/100,000 were selected as a study sample in Southwest China and another three provinces, Jiangsu, Zhejiang and Anhui province, with a low case detection rate of 0.023-0.042/100,000 were selected as a study sample in East China. Leprosy patients came from the family having household patients previously and registered from January 1, 1996 to December 31, 2005, were identified as index patients and were collected for analysis. The latest confirmed leprosy patients before the index patients in the same family were identified as the primary patients. Regarding the various terms of case detection methods, household contact survey means that every family member having a blood relationship to a patient with leprosy was checked up for whether or not she/he developed leprosy during the study period. The clue survey means that professional health workers collected leprosy suspects in the area reported by rural paramedical workers and checked up these suspects to confirm whether or not they had leprosy. A special questionnaire was designed, which included general information about the patient′s name, sex, age, residence, time of diagnosis of leprosy, clinical type, method of detection, bacterial index, number of previous patients within the family and time of diagnosis for household contacts, relationship between patients and relative, etc. The questionnaire was sent to each county unit responsible for leprosy control through the Provincial Center by mail. The questionnaires were filled in by health workers at the county level and then sent to the National Center for Leprosy Control through the Provincial Centers. All the data was tabulated and analysed using Statistical Program for Social Sciences (SPSS) software version 10.0 which was developed by SPSS INC, in Chicago, USA. Results A total of 2135 qualified index leprosy patients were collected from January 1, 1996 to December 31, 2005 in the study. Among them, 1998 index patients came from three provinces with a relative high prevalence rate in Southwest China and 137 patients from three provinces with a relative low prevalence rate in East China. Proportion of index patients among the newly registered patients Among all index patients, the male/female ratio was 1.96 and 1.32 and the Multibacillary patient (MB)/ Paucibacillary patient (PB) ratio was 2.74 and 3.28 in Southwest and East China, respectively. MB patients were defined as those with skin smear positive and the PB patients were defined as those with skin smear negative. The average age of the index patients at detection was 30.2 and 38.2 years in Southwest and East China, respectively. The mean delay time from onset of the disease to detection was 24.6 and 27.1 months, respectively, in both the areas. Methods of case detection among the index patients Proportion of index patients with multiple patients in the study The relationship between the index patients and the secondary patients Interval of case detection between index patients and primary patients Discussion In China, there was a report that when leprosy became low endemic, the household contact survey would be less cost effective. [1] However, there was a contrary report that in the low endemic area in Thailand, 62% of the newly detected patients had characteristics of contact. They concluded that a higher proportion of newly detected leprosy patients have a family history in a low endemic area compared with that in a high endemic area. [2] A study in Brazil [3] also reported that the lost patients among household contacts were at least four per every 10 new patients detected due to insufficient contact investigation. In our study, in Southwest and East China, new patients detected among leprosy household contacts accounted for 22.0 and 14.1% of the total newly detected patients, respectively, from 1996 to 2005 [Table - 1]. At the relatively high leprosy endemic area in Southwest China, the active household contact survey was a main case-finding method, which accounted for 36.1% of all household contact patients, which was higher than other detection methods. At the relatively low endemic area in East China, the skin clinic was a main case detection method, which accounted for 62.0% of all contact patients, and the proportion of the contact survey reduced to only 9.5% of all contact patients. However, the mean delay time from onset of disease to diagnosis was 27.1 months, which was longer than that detected in the high endemic area (24.6 months). It suggests that there was a delay in case finding among the household contacts in East China. It is known that leprosy is a chronic infectious disease. Transmission among household contact is closely associated with the age at contact, the clinical classification of the patients and physical and genetic constitution. [4] The household contacts of MB patients had a high risk of developing disease. [5] It was reported that among the 506 index patients reported in Brazil, 226 patients had a contact with a known patient, which accounted for 44.7%. Among them, 92 were household patients, which accounted for 18.2% of all patients.[6] In our study, the household patients accounted for 14.1-22.0%, which was similar to that reported in a study in Brazil. Although the household patients were a small proportion among newly detected patients, many researchers suggested that social contacts of leprosy should also be investigated, [5] especially for those living in the vicinity of a seropositive patient. Through testing the serological status of contacts and using a broader definition of contacts, higher risk groups of contacts could be identified. [7] The childhood leprosy is a sensitive indicator of the disease transmission. It can occur everywhere, at a high or low leprosy endemic situation, as long as there was an infectious source in the family. A report in India showed that of the 306 child patients, 113 (36.9%) had a history of family contact with leprosy.[8] However, if isolated from their parents affected by leprosy, very few children would suffer from leprosy. It was supported by a report from India, which stated that in 77 children staying away from their parents affected by leprosy for 6 months-6 years, nobody showed any symptom of leprosy. [9] Because leprosy has insidious clinical evolution without obvious symptoms at the early stage, many patients would not be aware of suffering from leprosy themselves and not see a doctor early. This may be a reason why there were so many patients with disability detected at the low endemic situation, and the child patients were also detected at the same time in China. [10] When analyzing the relationship between the index patients and the primary patients in our study, there seemed to be no big difference between Southwest and East China. The parents of the index patients, as the primary patients, had a maximal proportion, which accounted for 60.2%. The brother/sister of the index patients accounted for 17.3%, which ranked second. This indicates that there should have been more new patients developing among children of the index patients, the case detection focusing on this population. One of the reasons for some researchers questioning the value of household contact survey was that there was too long an interval between the detection of primary patients and the index patients. They argued that the long-term follow-up of the leprosy household contacts only detected a very few patients and it would also increase the discrimination toward leprosy. [1] But, there was a report that in high endemic areas in Indonesia, the mean duration from the primary patients to the index patients was 3 years and 95% of the index patients could be detected 6 years after registration of the primary patients. [11] Also, there was a report that a maximum number of patients acquired the disease during 0-6 years of contact. [12] In our study, the mean interval between the primary patients and the index patients was 15.8 years. This seemed to be longer than that reported in other countries. But, within 5 and 10 years, 24.2 and 43.7% of all index patients had been detected respectively by various case-finding methods in the study [Table - 2]. Considering that the delay time between onset and diagnosis of disease among index patients was more than 2 years, if these patients were followed-up intensively within 5 or 10 years, the proportion of detection would increase. Many index patients had indeed been detected more than 10 years after the primary patients. It is very important to strengthen the leprosy health education for the leprosy household contacts to encourage them to do self-reporting once they get suspect symptoms and signs of the disease. It was also recommended by some authors in India. [13] To believe that contact survey could increase the stigma toward patients, this is a really wrong conception. It is just a high-quality medical service to be provided to the patient if performed properly because it is based on convenience and minimal economic loss to the patients. In many tuberculosis (TB) control programs, the household contacts of TB patients were also regarded as a high-risk population [14] and to be followed-up for detection of new patients. They found that the patients were less advanced than those found through passive case detection. [15] In Hong Kong, China, the household contact survey was also followed-up and considered to be a useful method in the detection of TB patients. [16] In our study, the index patients were not divided into MB and PB for analysis because the MB patients accounted for 87.9% of all newly detected patients in China. [17] There was also a report that household contact of PB patients had a higher risk of developing disease than suspected registers. [18] The most important factors in developing disease were closeness and intensity of the contact and inherited susceptibility. [19] We just focus on the role of household contact survey in the case finding at the low endemic situation. At this time, without the more effective measures to detect early patients, especially at the low endemic situation, the household contact survey is still a useful method for case detection in the leprosy control program. References
Copyright 2009 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv09043t2.jpg] [dv09043t1.jpg] |
| |||||||||

{kind=link}
{kind=link}