 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
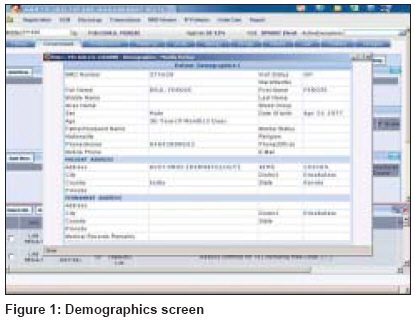
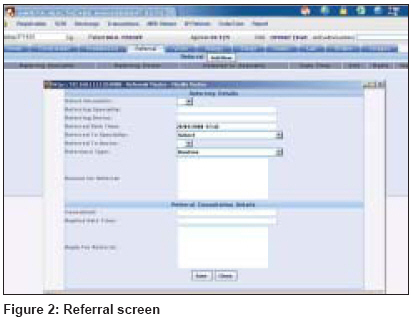
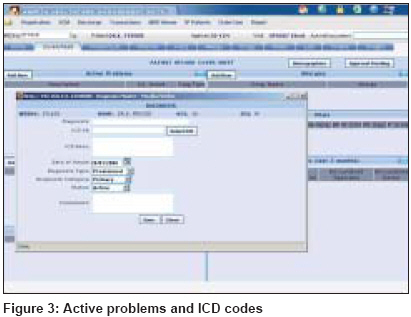
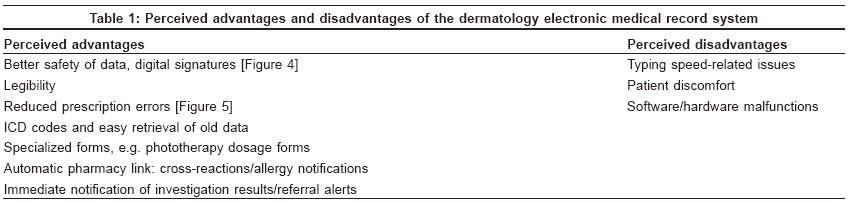
Indian Journal of Dermatology, Venereology and Leprology, Vol. 75, No. 2, March-April, 2009, pp. 157-161 Brief Report Electronic medical records in dermatology: Practical implications Kaliyadan Feroze, Venkitakrishnan S, Manoj Jayasree, Dharmaratnam AD Department of Dermatology, Amrita Institute of Medical Sciences and Research Centre, Kochi, Kerala Code Number: dv09044 Abstract Background: Electronic medical records (EMRs) can be of great use in dermatological data recording. Unfortunately, not many studies have been carried out in this specific area. Keywords: Electronic medical records, dermatology, time Introduction Electronic medical records (EMRs) can be of great use in dermatological data recording. There is a lot that EMR can offer to the betterment of dermatology services in any center. Unfortunately, not many studies have been carried out in this specific area. We attempt to evaluate the use of an EMR system in dermatology, comparing it with a conventional paper-based system.Methods Two hundred patient records of patients attending the Dermatology Outpatient Department during a 3-month period were included, which also included follow-up progress notes of the same patients. Half of these were entered totally in the electronic format while the other half were in the conventional paper format. Four doctors who were familiar with the EMR system (who were using the system for more than 3 months) were involved in entering the notes and the cases were randomized among them. None of the doctors had any special training in the use of computers. The EMR system used was the Amrita HISβ (Hospital Information System) developed indigenously by Amrita Enterprises, Kochi, India. The salient features of this EMR system include the patient demographics (which is entered automatically at the registration point), the patient case sheet [Figure - 1] (including history, examination findings, diagnosis, prescriptions and lab/service orders, which are entered by the dermatologist), lab reports, radiology images (entered by the corresponding lab service centers or radiology service centers), referral section [Figure - 2] (where referrals to other departments can be entered and replies to referrals made) and special fill boxes for allergies and entering the International Classification of Diseases (ICD) codes for diseases [Figure - 3]. Results Time Second visit progress notes were also studied. The average time taken for consultations and entering progress notes in the follow-up cases was slightly less than 10 min (9.7) for EMR while it was slightly more than 10 min (10.3) for the paper format. The difference was not statistically significant ( T -test, P -value > 0.05). We assume that this is partly because all previous investigation reports, X-rays, electro cardiograms and other data, like reply to referrals are all present on the patient coversheet itself and can be retrieved easily from the EMR system. The doctors involved mentioned that comparatively much more time was used in the EMR in entering prescriptions and diagnosis/ICD codes. Comparatively lesser time was used in the EMR for service ordering (like lab orders) and follow-up prescriptions (as there is an option for repeating the prescription with a single click). The difficulty of using multiple forms to fill in the patient details and required investigations for different categories, like serology, pathology or biochemistry, is avoided. To summarize, although the time taken for initial data recording in the EMR format is comparatively high as compared with the normal paper-based consultations, there are valid advantages in the EMR system, which more than make up for the time factor. Moreover, the time factor is significant only in the initial entry. In the follow-up cases, the EMR system actually fared favorably compared with the paper format. Some of the specific advantages and disadvantages of the EMR system that were noticed are summarized in [Table - 1]. Comfort Patient comfort: Contrary to expectation, there was not a single incident where the patient expressed any kind of discomfort with the dermatologist typing while taking a history. Discussion Not many studies have specifically targeted the application of EMRs in dermatology. One of the primary applications of EMR in dermatology was as part of teledermatology records. In fact, EMRs or patient information record was defined as all information pertaining to the patient for providing care using telemedicine. This includes clinical as well as non-clinical information. [1] However, as of now, EMR is used in the context of any medical record, not necessarily pertaining to telemedicine. One of the primary advantages as far as using EMR in dermatology is the fact that dermatology outpatients include a large number of chronic diseases with a follow-up duration of years. The advantage of a streamlined, one-click retrieval for old records as compared with a bulky paper file cannot be understated. The same applies to investigation and treatment charts for people on prolonged treatment schedules. Similarly, as dermatology patients are often on a long list of drugs and topicals, the ease of repeating only the necessary medication with a click of a button makes life easy for the dermatologist, especially as there is no question of losing old prescription notes. Most EMR implementation exercises show a gradual but steady increase in the acceptance rate as doctors become more familiar with the system. It should also be noted that a lot of the advantages of an EMR system come through only when all departments start using it at the same time. [2] Studies have shown that images are not used to track skin disease or integrated with EMRs nor are EMRs widely used, probably because of difficulty of use and limited computer literacy. [3] The issue of longer consultation times while using an EMR system has been studied by a number of authors. Most studies do not show a significant difference between adjusted average time for EMR and non-EMR consultations. [4],[5],[6] However, there needs to be a lot of further refinement before EMRs can become more the norm rather than an exception. With proper use, lifelong electronic health records can supply valuable information for research, quality management and health policies in addition to supporting the treatment of patients. [7] Further improvements/preferred additions in a dermatology-based EMR according to us would probably include features like:
In general, the future developments in EMR need to look more into the core needs of each specialty through the eyes of the health care professionals, patients as well as the health policies of the particular country. According to Hδyrinen et al , the challenge for ongoing national health record projects around the world is to take into account all the different types of EMRs and the needs and requirements of the different health care professionals and consumers in the development of EMRs. [8] The widespread implementation of health information technology in general has been limited by a lack of generalizable knowledge about what types of implementation methods will improve care and manage costs for specific health organizations. The reporting of health information technology development and implementation requires fuller descriptions of both the intervention and the organizational/economic environment in which it is implemented. [9] Although most studies show a positive patient response to EMRs, patient confidentiality and the ethical-legal issues associated with it (especially in the context of sexually transmitted diseases) may be another issue that needs to be looked at in detail. The requirement for patient consent in electronic records and the extent to which electronic patient data can be shared need to be delineated in clear terms, although a proper EMR system with good standards for authentication, authorization, auditing and accountability is likely to be more secure than a paper-based system. [10],[11],[12] The number of doctors using the system actively at our center at the time of submitting this article are too few to generalize the results. We also realize that the number of patients and time frame needs to be much larger to understand problems specific to dermatology in relation to an EMR system. However, we would like to reiterate that the aim of this report is merely to sensitise the readership to the potential of EMRs in dermatology and to stress on the point that each specialty has its own specific requirement as far as an EMR is concerned. Conclusion The use of an EMR system in dermatology (or for that matter in any specialty) may overawe most users at the beginning, but once a comfort level is established, EMR is likely to outscore conventional paper recording systems. The use of EMR routinely in dermatology clinics may be a long way away, but we feel that in the long run the advantages of such a system will be simply difficult to ignore. The linkage of long-term patient follow-up, including images to single-point retrieval, will really be useful in chronic dermatological diseases. A lot of user and software issues need to be ironed out before this becomes a reality. This article is basically meant only as a simple time-motion study, which aims to sensitize the dermatology readership to the potential of EMRs. It should be stressed that each specialty has its own needs when an effective EMR is to be designed. More detailed longitudinal studies are required to streamline the effective implementation of EMRs in dermatology.[Figure - 4],[Figure - 5]Acknowledgments To Br. Pradeep, CEO, Amrita Technologies, for his valuable support. To the technical staff involved in formulating and implementing the Hospital Information System in our hospital. The advantage of having people readily available for incorporating the doctors′ suggestions is one distinct advantage we enjoyed in our set up. To Dr. Ajit Babu, Director, Center for Digital Health, Amrita Institute of Medical Sciences, Kochi.References
Copyright 2009 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv09044f4.jpg] [dv09044f2.jpg] [dv09044f5.jpg] [dv09044f1.jpg] [dv09044t1.jpg] [dv09044f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}