 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
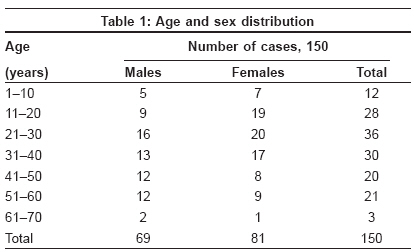
Indian Journal of Dermatology, Venereology and Leprology, Vol. 75, No. 2, March-April, 2009, pp. 162-166 Brief Report Evaluation of narrow-band UVB phototherapy in 150 patients with vitiligo Kumar YHari Kishan, Rao GRaghu Rama, Gopal K.V.T, Shanti G, Rao KVeerabhadra Department of Dermatology, King George Hospital/Andhra Medical College, Visakhapatnam, Andhra Pradesh Code Number: dv09045 Abstract Background: Very few studies have been performed to evaluate the efficacy and safety of narrow-band ultraviolet B (NBUVB) therapy in Indian patients with vitiligo and are of small sample size.Aims: The purpose of this study is to know the efficacy and safety of NBUVB in 150 vitiligo patients of various age groups. Methods: One hundred fifty patients (69 males, 81 females), aged 3-70 years, with vitiligo were treated twice weekly with NBUVB. The starting dose was 250 mJ/cm 2 in adults and 150 mJ/cm 2 in children, with 20% dose increments at each subsequent visit given for a maximum period of 1 year and were followed-up for 6 months for stability of repigmentation. Statistical methods were employed to establish the relation between the response and the number of exposures, duration of treatment, cumulative dose and the compliance. Results: Analysis of our study showed that a majority of our cases, about 73, achieved 25-75% repigmentation, with an average of 51 ± 19 exposures, 51 had <25% repigmentation, with an average of 19 ± 11 exposures and 26 had >75% repigmentation, with an average of 74 ± 24 exposures. Good response to therapy was directly associated with good compliance, more number of exposures and increasing cumulative dose, which was statistically significant (P < 0.01). Adverse effects were minimal. Only three patients developed depigmentation of repigmented sites during follow-up. Conclusion: Our study proves that NBUVB therapy is an effective and safe tool in the management of vitiligo, with good stability of repigmentation and cosmetic appearance. Keywords: Narrow-band ultraviolet B, Vitiligo Introduction Vitiligo still remains a difficult disease to treat, although various non-surgical and surgical treatment modalities have been mentioned in the literature. [1],[2],[3],[4] Psoralen with ultraviolet A (PUVA) therapy is a well-described therapy for vitiligo and is still the mainstay.[4],[5] Its limitations include acute side effects such as nausea and phototoxic reactions and long-term effects such as cataracts and carcinogenesis. Narrow-band ultraviolet B (NBUVB) is an emerging, effective and safe therapy for vitiligo. [4],[5],[6],[7] It is as effective as PUVA, without side effects. [8],[9] In 1997, Westerhof and Nieuweboer-Krobotova were the first to study the effect of NBUVB in vitiligo. [10] NBUVB therapy has also been reported to be safe in childhood vitiligo. [11] The clinical experience with NBUVB in vitiligo is limited, with very few reports published in the literature so far. Earlier reported studies were mostly in the western population and its experience in the darker race, including Indians, is limited. [7],[12],[13] In view of the paucity of experience with NBUVB, this large-scale study has been undertaken to evaluate the response pattern. Methods The study group included 150 cases of generalized and localized vitiligo. The study was prospective, open and non-randomised. One hundred fifty patients (69 males, 81 females) of vitiligo, with ages ranging from 3 to 70 years, were included. Patients with history of photosensitizing disorders, sensitive to photosol therapy and suffering from claustrophobia were not included. All these patients were advised to stop any previous treatment for at least 8 weeks before NBUVB monotherapy. A complete general and systemic examination was carried out to know the associated systemic diseases. A thorough dermatological examination was carried out taking note of the number of depigmented macules and the approximate percentage of body surface area involved using "Rule of Nine." Cases of vitiligo were classified as generalized and localized vitiligo. Relevant hematological and biochemical investigations were carried out in all the patients. Before starting NBUVB therapy, all the patients were taken around the phototherapy units and were counseled regarding the safety profile, the importance of adherence and compliance and limitations of therapy. Equipment used
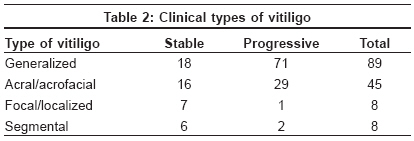
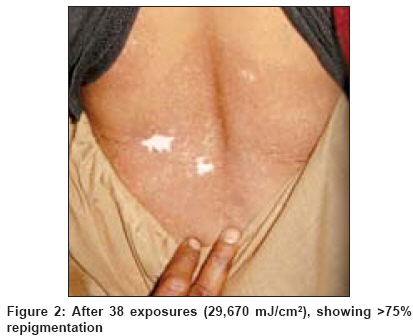
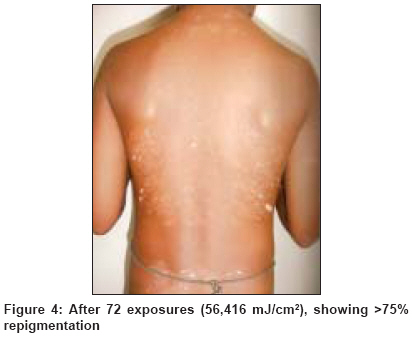
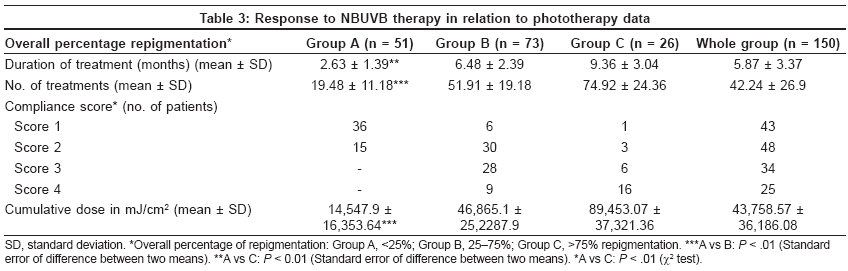
Treatment protocols of our center The maximum period of treatment was 12 months or earlier if 75% or greater repigmentation was achieved. Maintenance therapy once in a week for 4 weeks and once in 2 weeks for another 4 weeks was given. If there was no repigmentation even after 6 months of therapy, NBUVB was discontinued. All the patients were examined by the same dermatologist at 4-week intervals and lesional photographs were taken at baseline and thereafter to document the pattern and extent of repigmentation. All the patients were followed-up for 6 months after termination of therapy to observe the stability of repigmentation. Computerized phototherapy data of all the patients was maintained. The patients who responded to NBUVB therapy were grouped as Group A - < 25% repigmentation, Group B - 25-75% repigmentation and Group C -> 75% repigmentation. Response to treatment was assessed by comparing the photographs of before and after therapy. Patient compliance was scored as Score 1 - < 25 treatments, Score 2 - between 25 and 50 treatments, Score 3 - between 50 and 75 treatments and Score 4 - > 75 treatments. Statistical methods were employed to establish the relation between the response and the number of exposures, duration of treatment, cumulative dose and the compliance using the standard error of difference between the two means and the χ2 test, depending on the type of data set involved. Significance level was set at P < 0.01, which is statistically highly significant. Results Of the 150 patients, 69 (46%) were males and 81 (54%) were females and their ages ranged from 3 to 70 years [Table - 1]. The duration of disease ranged from 1 month to 28 years, with a mean duration of 14 years. Eighty-two (54.6%) patients had a duration of vitiligo of 5 years or less and 68 (45.4%) patients had a duration of vitiligo of more than 5 years. Twenty-eight (18.6%) patients had a family history of vitiligo, 20 (13.3%) patients had hypothyroidism and nine (6%) were with diabetes mellitus. Eighty-nine (59.3%) patients had generalized vitiligo, 45 (30%) patients had acral/acrofacial type, eight (5.3%) had focal and eight (5.3%) had segmental type of vitiligo [Table - 2]. Of the 150 patients, 27 (18%) received NBUVB therapy for 1 year. Ninety-eight (65%) patients had therapy for less than 12 months because of satisfactory repigmentation. Twenty-five (17%) abruptly stopped treatment even before achieving 25% repigmentation. Of the 150 patients, 51 (34%) had less than 25% repigmentation, 73 (48.6%) achieved 25-75% repigmenation and 26 (17.4%) had more than 75% repigmentation. Of these 26 cases, only five (3%) cases showed complete repigmentation [Figure - 1],[Figure - 2],[Figure - 3],[Figure - 4]. Certain anatomic sites responded better than others. The best response (i.e.> 75% repigmentation) was achieved with lesions located on the face and neck, followed by the trunk, back, arms and legs. The lesions over the knees, elbows and other bony prominences seldom showed more than 75% repigmentation. The lesions on the hands, digits, feet, toes and lips showed < 25% repigmentation. Patients with leukotrichia in the depigmented lesions were resistant to treatment. Repigmentation in a majority of the cases was follicular in nature and in a few, repigmentation occurred from the periphery. Most patients experienced that the initial repigmentation was darker. Few weeks later, in all the cases, the repigmented color matched well with the normal skin, giving a good cosmetic appearance. The disease activity had significantly decreased after NBUVB therapy. Before therapy, most patients, about 103 (68%), had active disease, whereas after therapy, the disease had stabilized in 90% of the cases and the remaining 10% continued to develop new lesions. The response to therapy was faster and good in children and those with a short duration of the disease. Statistical analysis of NBUVB therapy in relation to phototherapy data Side effects Follow-up Discussion Although PUVA therapy is a well-established first-line treatment for vitiligo, recent studies have shown that NBUVB therapy is more effective, less dangerous and superior to PUVA therapy. [4],[8],[9] NBUVB therapy is now a more or less established and recommended phototherapy for generalized vitiligo, pregnant women and children because of the high safety profile. [4],[11],[13] Determination of minimal erythema doses (MED) is essential for rational treatment with UV light. Serish and Srinivas reported that the mean MED for NBUVB was 300 mJ/cm 2 for the Indian skin. [16] In the present study, although MED was not calculated, the NBUVB therapy was started with an initial dose of 250 mJ/cm 2 . The optimal NBUVB irradiation regimen has yet to be defined. Hence, large-scale studies are warranted to establish the standard protocol of NBUVB therapy. In this particular study, lesser number of exposures (51.91 ± 19.18) were required to achieve 25-75% repigmentation. Similarly, the cumulative dose was also lesser (46.8 ± 25.2 J/cm 2 ) to achieve the same repigmentation, whereas Njoo et al. [11] reported the same repigmentation with more number of exposures (76.3 ± 16.7). The same observations were reported in other western studies. [6],[8],[11],[14],[15] Our study and other Indian studies [7],[12],[13] showed that dark skin (Fitzpatrick type IV and V) requires lesser number of exposures and cumulative dose to achieve 25-75% repigmentation when compared with white skin (Fitzpatrick I and II). It has also been observed in our study that with good adherence to therapy and compliance, faster and good response can be achieved. It has been proved statistically that good response is directly associated with more number of exposures, cumulative dose and good compliance. We have also observed during the course of therapy that initially, in some patients, newer lesions used to develop but while continuing the therapy, newer lesions cease to appear and the disease was stabilized. This could be due to the immunomodulatory effect of NBUVB, although the precise mechanisms are still not known. In our study also certain anatomical sites like face, neck, trunk and back responded faster, with better repigmentation to NBUVB therapy, and poor response was observed over the acral areas. The repigmentation achieved in all the cases was cosmetically accepted and matched with the surrounding normal skin, unlike in PUVA therapy. In this way, NBUVB therapy is superior to oral PUVA therapy. In our study panel, NBUVB equipment was used in children and in patients with localized vitiligo. This particular NBUVB equipment was found to be useful and handy, particularly in the pediatric age group and similar results were obtained. It has been observed that children responded faster with good repigmentation (> 75%), with lesser number of exposures and cumulative dose of NBUVB. Similar observations were reported in other studies also. Lahiri et al. found that NBUVB therapy was a useful tool in inducing repigmentation after regrafting in punch-grafting failure cases. [17] The same authors also reported successful repigmentation of lip vitiligo with punch grafting combined with NBUVB therapy. [18] The adverse effects in our study were minimal and none of the patients required discontinuation of therapy. The adverse effect profile observed in our study was similar to that reported in the literature. [4],[5],[6],[7],[8],[11],[15] All these studies, including ours, clearly establish the safety profile of NBUVB therapy. During the follow-up period of 6 months, of the 150 patients, only three patients developed depigmentation of repigmented sites. However, long-term follow-up is needed to observe stability of repigmentation. Conclusions Our study, like all other studies, establishes that NBUVB therapy is an effective and safe modality to treat vitiligo of all age groups with cosmetically acceptable repigmentation. Adherence and good compliance are pre-requisites for this therapy to achieve satisfactory repigmentation. Therefore, all the patients are properly educated and counseled on these lines before offering NBUVB therapy.References
Copyright 2009 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv09045f4.jpg] [dv09045f2.jpg] [dv09045t3.jpg] [dv09045t2.jpg] [dv09045f3.jpg] [dv09045t1.jpg] [dv09045f1.jpg] |
| |||||||||


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}