 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
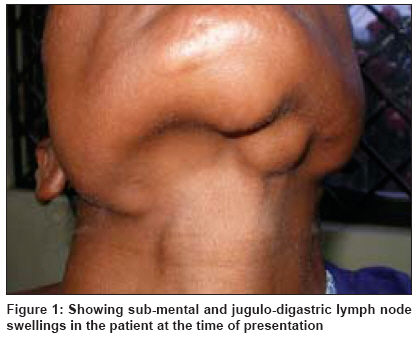
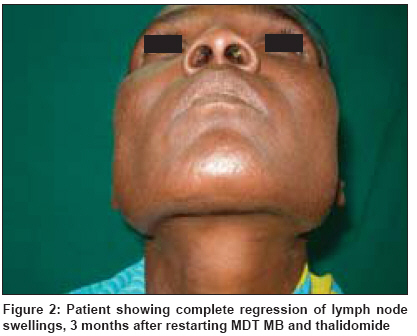
Indian Journal of Dermatology, Venereology and Leprology, Vol. 75, No. 2, March-April, 2009, pp. 177-179 Case Report Relapse of leprosy presenting as nodular lymph node swelling Kiran KU, Krishna Moorthy KV, Meher Vani, Rao PNarasimha Department of Dermatology, Bhaskar Medical College, Hyderabad Code Number: dv09049 Abstract Lymphadenopathy is known to be associated with lepromatous leprosy and has also been observed as a feature of type-2 lepra reaction. However, nodular lymph node enlargement is not commonly reported in leprosy patients or as a feature of relapse. We herewith are presenting a case of bacteriological relapse in a patient of lepromatous leprosy treated 22 years before till smear negativity with WHO multidrug therapy (MDT) multibacillary type (MB). She presented with prominent nodular swelling of the cervical group of lymph nodes along with generalized lymphadenopathy, which was mistakenly treated as tubercular lymphadenopathy. A diagnosis of late bacteriological relapse of lepromatous leprosy presenting with prominent lymphadenopathy and ENL was made after relevant investigations. The patient was started on treatment with WHO MDT MB (daily dapsone and clofazimine and monthly rifampicin) and thalidomide (200 mg/day). Nerve pain regressed within 2 weeks of therapy. The lymph nodal swelling regressed within 3 months of starting treatment.Keywords: Lymph node swelling, relapse of leprosy Introduction The introduction of multidrug therapy (MDT) in the treatment of leprosy had a favorable effect with a reduction in the relapses that were common among patients treated with dapsone monotherapy. Nonetheless, they are still reported even among multi bacillary (MB) patients treated with 24 months of WHO MDT regimen and also in those treated till smear negativity. [1],[2] Relapses in leprosy are biphasic: early relapses resulting from inadequate therapy while late relapses may be the outcome of reactivation of persisters or re-infection. [3] Relapse is usually associated with the rise in the bacteriological index (BI) and/or a positive morphological index (MI), [4] with or without the appearance of fresh lesions in a treated patient of leprosy. The relapse rate with reference to the time gap after "release from treatment (RFT)" reveals that relapse declines with passage of time after RFT, with a majority of relapses occurring in the first 3 years after RFT. [5] Lymphadenopathy is known to be associated with lepromatous leprosy and has also been observed as a feature of type-2 lepra reaction. Mycobacterium leprae have been isolated from lymph nodes in lepromatous leprosy patients treated with MDT MB for 24 months. [6] However, nodular lymph node enlargement is not commonly reported in leprosy patients or as a feature of relapse. We are presenting a case of bacteriological relapse in a patient of lepromatous leprosy treated 22 years before till smear negativity with WHO MDT MB. She presented with prominent nodular swelling of the cervical group of lymph nodes along with generalized lymphadenopathy, which was mistakenly treated as tubercular lymphadenopathy. Case Report A female of 40 years presented with erythema nodosum leprosum (ENL) lesions on the extremities associated with bilateral cervical lymphadenopathy to our clinic. She gave a past history of having completed MDT MB at a leprosy center and was released from treatment in the year 1985 after she became smear-negative. The patient gave a history of recurrent ENL reactions, on and off, over the last several years and was on oral corticosteroids apart from other supportive measures for its management. In the year 2006, she developed generalized lymphadenopathy with prominent nodular enlargement of the cervical lymph nodes. A diagnosis of tubercular lymphadenitis was initially made based on fine-needle aspiration cytology (FNAC) of the cervical lymph nodes and the patient was put on 6 months of antituberculous treatment. However, she did not respond to the therapy, showing no reduction in the cervical lymph node swelling. The patient presented to us in August 2007 with a persistent visible nodular cervical lymph node swelling [Figure - 1] and ENL lesions on the upper and lower limbs associated with fever. No hypopigmented macules or patches were observed. Other lymph node groups enlarged were bilateral inguinal, epitrochlear and axillary lymph nodes. All the groups of lymph nodes were firm and non-tender. Both ulnar nerves were thickened and tender. With this background, we investigated this patient. Routine investigations were within normal limits and screening for syphilis and human immunodeficiency virus was negative. Skin smear was positive for acid-fast bacilli (AFB), with an average bacteriological index (BI) of 3.6 and morphological index (MI) of 0.6. Skin biopsy revealed lepromatous leprosy and the BI of granuloma was 3. A second FNAC from the lymph node showed numerous AFB on modified Ziehl Neelsen (ZN) stain. On inoculating the aspirate from the cervical lymph nodes on Lowenstein Jenson′s (LJ) medium, no growth of M. tuberculosis was observed even after 8 weeks. When a specific polymerase chain reaction (PCR) was performed from the aspirate of the lymph nodes, it was positive for M. leprae and was negative for M. tuberculosis. A diagnosis of late bacteriological relapse of lepromatous leprosy presenting with prominent lymphadenopathy and ENL was made based on the above findings. The patient was started on treatment with WHO MDT MB (daily dapsone and clofazimine and monthly rifampicin) and thalidomide (200 mg/day). Nerve pain regressed within 2 weeks of therapy. The lymph nodal swelling regressed within 3 months of starting treatment [Figure - 2]. Discussion Generalized lymphadenopathy as a leading feature is a rare type of presentation of relapse in a patient of leprosy. The patient in the present report was treated with a full course of MDT MB 22 years back till smear-negativity. In fact, her skin smear status was observed to be persistently negative in the three follow-up smear examinations after RFT. The presentation of this patient in the year 2006 with prominent cervical lymph node swelling made the treating physician consider it as tubercular lymphadenopathy based on the positive AFB in the FNAC aspirate and she was treated with antitubercular therapy. It should be noted that in the modified ZN staining, it is difficult to differentiate between M. tuberculosis and M. leprae bacilli. Moreover, such a presentation of tubercular cervical lymphadenopathy is quite common in India, which is endemic for tuberculosis. Concomitant lepromatous and tuberculosis infections involving lymph nodes have been reported [7] apart from tubercular lymph node involvement in patients of leprosy. [8] However, negative PCR, no growth on LJ medium and non-response to antitubercular therapy ruled out tuberculosis as a cause of lymphadenopathy in this patient. Lymph node involvement in leprosy is well documented in leprosy patients. The frequency of lymph node involvement reported in an Indian study was inguinal 76.2%, cervical 69.5%, axillary 69.5%, epitrochlear 64.7% and pre-auricular 9.5%. [9] M. leprae were reported from lymph node aspirates of leprosy patients. [10] It was also reported that non-caseating granulomas and M. leprae were observed in the lymph node biopsies in nine of the 11 lepromatous leprosy patients after completion of 2 years of MDT MB therapy. [6] In another study, in 26 patients of tuberculoid (TT) leprosy, 11.54% showed presence of AFB in lymph nodes and in 18 patients of borderline tuberculoid (BT) leprosy, 61.1% showed granuloma and 11.11% showed presence of AFB in lymph nodes. [11] In our patient, the possibility of re-infection cannot be ruled out. However, history of recurrent ENL reactions over the years points to the possibility of relapse rather than re-infection. Corticosteroids given for recurrent ENL over the years in this patient might have contributed to the persistence of M. leprae infection. Often, lepra reactions are associated with the presentation of relapse. [1] The recurrence of ENL even after 20 years of RFT after smear negativity and absence of stringent laboratory evidence of tuberculosis made us suspect and investigate this patient for the possibility of relapse of leprosy. The BI of 3+ with MI positivity in skin smears along with presence of M. leprae and absence of M. tuberculosis -specific DNA product on PCR from the lymph node aspirate confirmed the relapse of leprosy. Conclusions We are presenting this case for the atypical presentation of relapse of leprosy with nodular lymph node swelling of the submental and cervical lymph nodes mimicking tubercular lymphadenopathy in a patient treated with MDT MB about 22 years back till smear-negativity.References
Copyright 2009 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv09049f2.jpg] [dv09049f1.jpg] |
| |||||||||

{kind=link}
{kind=link}