 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
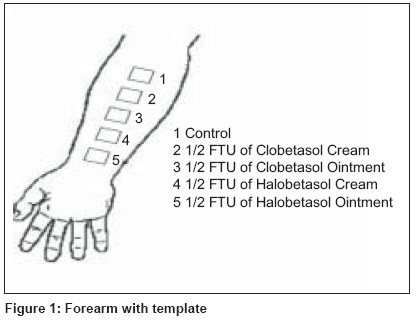
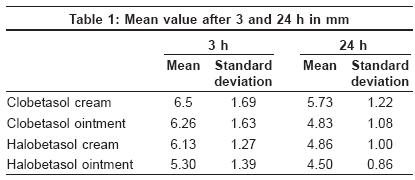
Indian Journal of Dermatology, Venereology and Leprology, Vol. 75, No. 2, March-April, 2009, pp. 186-187 Letter to the Editor Halobetasol versus clobetasol: A study of potency Mohandas Soumya, Rai Reena, Srinivas CR Department of Dermatology, PSG Hospitals, Peelamedu, Coimbatore-641 004 Code Number: dv09055 Sir, Topical corticosteroids (TCS) are an integral part of dermatological therapeutics. The clinical effects of TCS depend on the structure of the molecule, the vehicle and the skin onto which it is applied. [1] Addition of a fluorine molecule at six and/or nine positions enhances the potency of TCS. Halobetasol propionate has 6a flouro clobetasol 17-propionate as the active ingredient. Very occlusive vehicles enhance TCS molecule percutaneous absorption probably by increasing the hydration of the stratum corneum. [2] To estimate potency, various assays like vasoconstrictor assay and artificially induced inflammation using ultraviolet light can be used. [1] The ability of TCS to inhibit the size of histamine-induced wheal was used to assess the relative efficacy of halobetasol propionate and clobetasol 17-propionate in cream and ointment formulations in an open-labeled study conducted on 30 volunteers. Thirty volunteers who had not used systemic, topical corticosteroids or antihistamines for at least 8 weeks and not on any other drugs for at least 7 days were studied. Pregnant and lactating females, individuals with history of any atopy, systemic disease or skin infection were excluded from the study. A template with five apertures (3 cm x 3 cm) cut 2 cm apart was placed on the left forearm and, with a marker pen, each aperture was outlined. The squares were numbered 1, 2, 3, 4 and 5. The first aperture was left free. A half fingertip unit each of halobetasol ointment and cream and clobetasol ointment and cream was applied over apertures 2, 3, 4 and 5, respectively [Figure - 1]. The first square and steroid preparations on all the other squares were wiped after 3 h with a dry gauze piece. Prick testing was performed on all squares by the standard method. A drop of 0.1% w/v histamine solution was placed on the test sites and the skin was pricked through the histamine solution with a lancet. The tip was kept parallel to the skin surface and the skin was lifted by tenting the lancet by 45-60°. After 1 min, the test sites were dabbed with filter paper to remove excess histamine solution. The size of the wheal was recorded in millimeters after 15 min and the mean size was calculated by measuring the maximum diameter and the orthogonal diameter of the wheal with a transparent scale. Similarly, prick testing was carried out after 24 h. The mean diameter of the wheal after 3 and 24 h is shown in [Table - 1]. Post hoc analysis showed that at 3 h there was a statistically significant difference in wheal suppression between clobetasol cream and halobetasol ointment ( P = 0.005), clobetasol ointment and halobetasol ointment ( P = 0.015) and halobetasol cream and halobetasol ointment ( P = 0.035). Maximum wheal suppression at the end of 3 h was seen with halobetosol ointment followed by halobetosol cream whereas wheal suppression was least with clobetasol cream. At 24 h, the difference in wheal suppression between clobetasol ointment and halobetasol cream and halobetasol ointment were not statistically significant. However, there was a statistically significant difference in wheal suppression between clobetasol cream and clobetasol ointment ( P = 0.001), clobetasol cream and halobetasol cream ( P = 0.002) and clobetasol cream and halobetasol ointment ( P = 0.000), which was statistically significant. At the end of 24 h, there was no statistically significant difference in wheal suppression between halobetosol ointment, cream and clobetasol ointment, but clobetasol cream was the least effective. Halobetasol is a super-potent TCS with additional fluorine at the 6a position when compared with clobetasol. The additional fluorine in the 6a position further increases its topical anti-inflammatory and anti-proliferative activities. [3] In pre-clinical investigations, halobetasol propionate was superior to clobetasol 17 propionate with regard to its anti-inflammatory, vasoconstrictive and anti-proliferative effects. [4] In a double-blind, parallel-group, multicenter trial in 134 patients with severe, localized, plaque psoriasis, the success rate at the end of the study was 96% in the halobetasol propionate group and 91% in the clobetasol propionate group This added potency was attributed to additional fluorine in halobetasol. [5] Recent studies have shown that additional fluorine in halobetasol may not add to the potency. It was concluded that the presence of additional halogen substitutions does not necessarily result in increased potency. [6] In our study, we took 3 h measurements because the maximum wheal suppression occurs at the end of 3 h. [7] Twenty-four hour reading was taken to compare the potency of halobetasol and clobetasol at the end of 24 h. In this study, we found that at the end of 3 h halobetasol is more potent than clobetosol, ointment preparation being more potent than cream. At the end of 24 h, there was no statistically significant difference in potency between halobetasol and clobetasol except for clobetasol cream, which was found to be less potent. References
Copyright 2009 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv09055t1.jpg] [dv09055f1.jpg] |
| |||||||||


{kind=link}
{kind=link}