 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
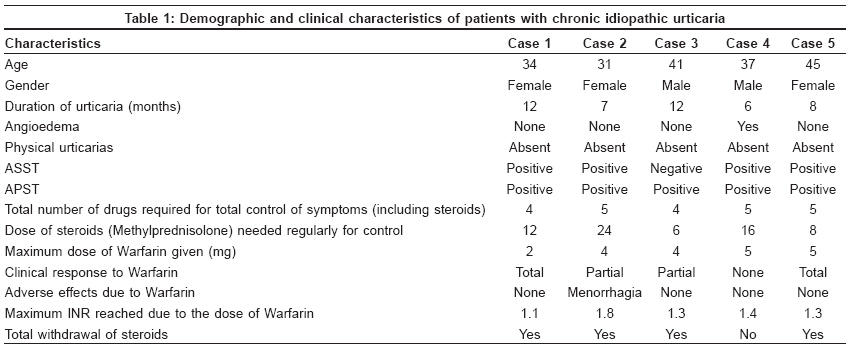
Indian Journal of Dermatology, Venereology and Leprology, Vol. 75, No. 2, March-April, 2009, pp. 187-189 Letter to the Editor Effect of warfarin on chronic idiopathic urticaria Mahesh PA, Pudupakkam VedanthanK, Holla AmruthaD, Dande Tejaswini Department of Pulmonology, JSS Medical College and Hospital, Mysore Code Number: dv09056 Sir, Urticarias unresponsive to antihistamines are frustrating for both physicians and patients. In severe cases, steroids or cyclosporine may be needed. [1] This retrospective observation highlights the potential of warfarin in managing chronic idiopathic urticaria (CIU). Five patients with CIU needed daily oral steroids for more than 3 weeks, with symptom recurrence on tapering steroids at least twice. Literature search for drugs that could be useful identified warfarin, which had shown benefit in managing CIU unresponsive to antihistamines. [2] A detailed history was followed by an autologous serum skin test (ASST) and an autologous plasma skin test (APST). [3] None had any pre-disposition to bleeding nor were on medications that interacted with warfarin. Baseline coagulation parameters were normal. Warfarin was initiated at 1 mg and increased by 1 mg weekly, with adequate monitoring of prothrombin time (PT) [Table - 1]. Dosage was maintained in symptom-free patients with tapering of steroids. Steroids were tapered every 3 days. Response was evaluated by physician examination every week and was graded as "none," "partial" and "total." "None" included no difference in the number, duration and size of wheals and severity of itching. Lesser extent of urticaria in the preceding week was considered "partial" and having no urticaria in the preceding week, "total." Demographic and clinical characteristics are summarised in [Table - 1]. All five cases had positive APST and four had positive ASST. In four cases, steroids could be withdrawn completely. Warfarin was used for 2-5 months. In three patients, there was no recurrence of CIU after warfarin withdrawal. Two patients, with onset of clinical response within 2 weeks, had "total" response, possibly due to warfarin. Two had "partial" response at 2 months, in whom it was difficult to differentiate the effect of warfarin from steroids. In one, no reduction in clinical symptoms or steroids was possible. We are aware of only one communication regarding the use of warfarin in difficult-to-treat autoreactive CIU. In the study by Parslew et al, [2] APST was not performed and patients were ASST negative. In our patients, APST was positive in all and ASST in four and the international normalized ratio (INR) was below 2 in all patients, whereas Parslew et al [2] maintained an INR between 2 and 2.5 to obtain benefit from warfarin. Warfarin dosage of 2-5 mg was similar to the study by Parslew et al (2-6 mg). The mechanism of action of warfarin is by suppression of thrombin, a potent mast cell degranulator, [4] and proteins in the coagulation cascade (Factors VII, IX and X). [3] Asero et al demonstrated involvement of the extrinsic coagulation pathway in CIU [5] thus providing the rationale for anticoagulant use. Monitoring patients with PT repeatedly is important as the major adverse effect is bleeding, especially with an INR of more than 3. Some drugs potentiating warfarin include fluconazole, omeprazole, metronidazole, acetaminophen, cotrimoxazole and antiretroviral drugs like protease inhibitors. Caution should be exercised in patients using other antiplatelet drugs like aspirin or non-steroidal anti-inflammatory drugs. Prospective long-term studies with adequate design are required to place warfarin appropriately in the management of CIU. Characteristics of subjects responsive to warfarin as compared with non-responders, monitoring D-dimer levels and risk-benefit ratio need elucidation. Warfarin may be useful in autoreactive CIU. Warfarin may be considered in subjects with CIU with coexisting diseases needing long-term warfarin, like deep vein thrombosis, atrial fibrillation or recurrent pulmonary embolism. References
Copyright 2009 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv09056t1.jpg] |
| |||||||||

{kind=link}