 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
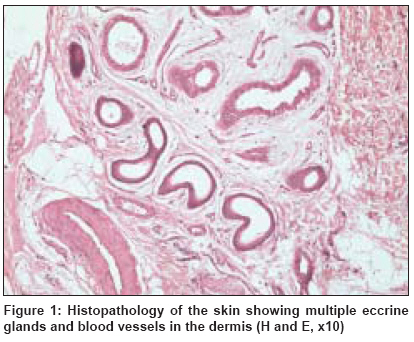
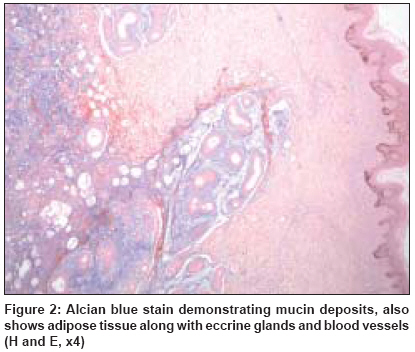
Indian Journal of Dermatology, Venereology and Leprology, Vol. 75, No. 2, March-April, 2009, pp. 193-194 Letter to the Editor Eccrine angiomatous hamartoma in an adult Natarajan Karthika, Rai Reena, Sundararajan Vanita, Venkatchala Sandhya Department of Dermatology, PSG Hospitals, Peelamedu, Coimbatore - 641 004 Code Number: dv09060 Sir, A 37-year-old female presented with a single bluish painful nodule over the midcalf of the left leg for 2 years, which was gradually progressing in size. The patient did not have any systemic problems and denied history of similar lesions in other members of the family. On examination, a well-circumscribed single violaceous nodule measuring 1 cm x 1.5 cm was found, which was tender on compression. Differential diagnoses considered were dermatofibroma, eccrine nevus and smooth muscle hamartoma. Surgical excision revealed a tissue of fibroelastic consistency. Histopathology revealed multiple well-circumscribed unencapsulated nodules in the deep dermis and subcutis. Nodules were composed of eccrine glands and blood vessels with mucinous stroma and fat cells around the glands, which was diagnosed as eccrine angiomatous hamartoma (EAH) [Figure - 1] and [Figure - 2]. EAH is a rare, benign cutaneous tumor usually present at birth or during early infancy and childhood. [1],[2] There are few references of lesions that have appeared in adult life or in puberty, [3] such as described in this case report. Clinically, EAH presents as an angiomatous lesion, usually solitary, although cases with multiple lesions have been described. [1],[2] Clinical manifestations may vary from nodules to plaques of erythematous bluish or brownish color or verrucous lesions. They may be located in any part of the body, although, they are more frequently found in the palmoplantar regions. [4],[5] EAH, generally asymptomatic, may present with focal hyperhidrosis and pain that is spontaneous or follows local pressure. The pain occurs due to involvement of nerve fibers and hyperhidrosis is because of the stimulation of the eccrine components, caused by the elevated local temperature within the angioma. [6] On histopathology, EAH is characterized by a dermal proliferation of well-differentiated eccrine secretory and ductal elements closely associated with thin-walled angiomatous channels. [7] Pilar structures may sometimes be involved. [8] In addition, unusual histopathologic variants have been reported and include the infiltration of the adipose tissue [8],[9] and increased dermal mucin, [8] as was found in our case. Immunohistochemical study (not performed in this case) can demonstrate that antigens frequently found in eccrine glands, such as the carcinoembryonic antigen and protein S-100, are reduced qualitatively in the eccrine glands of EAH, while Ulex europaeus , CD34, CD44 and the antigen related to factor VIII are expressed by the endothelial cells of the vascular components. [10] The differential diagnosis of EAH may include an eccrine nevus, tufted angioma, vascular malformations, macular telangiectatic mastocytosis, nevus flammeus, glomus tumor and smooth muscle hamartoma. These entities can be differentiated by histopathology. [11] The natural history of EAH is benign and typically slow-growing and hence aggressive treatment is generally unwarranted. Simple excision is usually curative and is reserved for painful or cosmetically disfiguring lesions. [7] In our patient, the excision proved to be curative and the patient is asymptomatic. We report this case for the rarity, occurrence in adulthood and the presence of adipose tissue and mucin, which is an unusual histopathological variant. References
Copyright 2009 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv09060f2.jpg] [dv09060f1.jpg] |
| |||||||||

{kind=link}
{kind=link}