 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
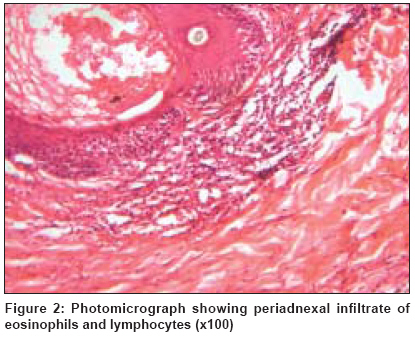
Indian Journal of Dermatology, Venereology and Leprology, Vol. 75, No. 2, March-April, 2009, pp. 194-196 Letter to the Editor Doctor I am on fire: Eosinophilic folliculitis in HIV negative Suresh MS, Arora Sandeep, Nair R.R.K Department of Dermatology, 5 AFH C/O 99 APO Code Number: dv09061 Sir, Eosinophilic folliculitis (EF) is a recurrent cutaneous eruption, usually intensely pruritic, of unknown etiology. It was initially described in 1965 by Ise and Ofuji, who reported a case of recurrent follicular pustules and eosinophilia in a Japanese woman.[1] Since then, it has been variously described as eosinophilic pustular folliculitis, sterile eosinophilic pustulosis and Ofuji disease. A 55-year-old, extremely restless man presented to us with complaints of a third episode of an intensely itchy rash over his scalp, face, upper extremities and trunk in as many years. He had been experiencing recurrent eruptions of severely itchy lesions over the affected areas for the past 3 years, with no specific seasonal variation. There was no history of vesiculation or oozing from the lesions, known allergies or drug intake before each episode of the rash. The individual typified his complaints as "I am on fire." He had been managed in the past with 5% permethrin, 1% gamma benzene hexachloride and antihistaminics, with no relief. The rash would subside with a short course of systemic steroids to recur again later. On examination, the individual was restless enough not to be able to sit still and appeared in acute discomfort. There were multiple folliculocentric papules and few pustules in a generalized distribution over his face, upper extremities and trunk in a supraumbilical distribution along with multiple excoriations [Figure - 1]. The scalp had a few similar lesions. The palms, soles, genitalia and flexures were spared. Investigations revealed a normal hemogram, erythrocyte sedimentation rate (ESR) of 8 mm at the end of 1 hour and an absolute eosinophilic count of 830/mm 3 . The serum immunoglobulin (Ig) E level was 11,302 IU/L. The biochemical profile was normal. The enzyme-linked immunosorbent assay for human immunodeficiency virus (HIV) antibodies and markers of chronic hepatitis were negative. Gram stain from the few pustular lesions did not reveal any organisms and the bacterial culture was sterile. Histopathology revealed a normal epidermis with an intense dermal infiltrate around the hair follicles and sebaceous glands consisting of aggregates of eosinophils and lymphocytes [Figure - 2]. The patient was managed with oral prednisolone 60 mg/day, dapsone 100 mg twice a day and pheniramine maleate 25 mg at night. At the end of 48 hour, he reported symptomatic improvement with reduction in itching and discomfort. After a week, the systemic steroids were discontinued and he was continued on oral dapsone 100 mg twice a day for another month. He now remains symptom-free at the end of 6-months of follow-up. EF is a recurrent itchy papulopustular eruption of obscure etiology, which occurs more commonly in males, in the third to the fifth decade of life. Although production of cytokines and chemotactic factors and expression of intercellular adhesion molecules are evidence of activation of the follicular sebaceous unit, the stimuli that provoke these changes are unknown. Immunological, infectious as well as environmental factors have been considered to play a role in the etiology. [2] The eruption is typically distributed in the supraumbilical areas and involves the face in 85% of the cases, although atypical forms have been reported. [3] It typically appears as an area of erythematous papules and pustules, which gradually become confluent, creating indurated polycyclic plaques with a healing center and spreading periphery. They ultimately fade away, leaving residual hyperpigmentation and scaling. Infantile EF is characterized by erythematous papulopustules on the scalp as the primary area of involvement. HIV-associated EF classically presents as recurrent, pruritic, erythematous or urticarial follicular papules located on the upper body. In these patients, it may be a marker for a high risk of developing opportunistic infections as they usually appear at a CD4 count of < 250/µL. EF has also been reported in association with chronic hepatitis infection and drug intake. [4] Management of EF has been variously described in the literature, with steroids being the mainstay of therapy. Other modalities include topical corticosteroids, oral itraconazole, isotretinoin, phototherapy, colchicine, minocycline, acitretin, cyclosporine A, UV-B therapy, interferon alfa-2b, tacrolimus, doxycycline and radiation therapy. [5] Our patient was an otherwise healthy male in the sixth decade who had repeated episodes of EF with multiple crops of papules and pustules in a folliculocentric distribution. He was HIV negative and did not volunteer any history of regular intake of any medication in the past. The basis of diagnosis was the clinical profile, peripheral eosinophilia, an elevated serum IgE level and the histopathology. EF is considered a rarity outside Japan. The few cases seen nowadays are more commonly associated with HIV infection. Our case was HIV negative and had no associated positive history suggestive of a possible aggravating factor. The case is hence reported for its rarity and for successful management with dapsone, which otherwise has been used sparingly in this condition. References
Copyright 2009 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv09061f2.jpg] [dv09061f1.jpg] |
| |||||||||

{kind=link}
{kind=link}