 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
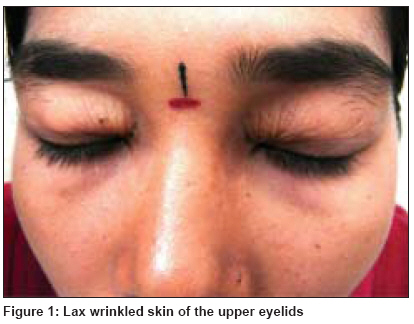
Indian Journal of Dermatology, Venereology and Leprology, Vol. 75, No. 2, March-April, 2009, pp. 197-199 Letter to the Editor Blepharochalasis Mercy Polavarapu, Ghorpade Ashok, Das Manabendra, Soud Abdulla, Agrawal Shruti, Kumar Ashok Department of Dermatology, Venereology and Leprosy, J.L.N Hospital and Research Centre, Bhilai-490 006, Chhattisgarh Code Number: dv09063 Sir, Blepharochalasis is a rare degenerative disease of the skin of the eyelids, characterized clinically by bilateral or unilateral swelling followed by laxity, atrophy, wrinkling and pigmentary changes, predominantly of the upper eyelids. [1] The skin of the eyelids becomes so lax that it droops as redundant folds over the lid margins. [2] The term blepharochalasis was first coined by Fuchs in 1869, meaning eyelid relaxation in Greek. [3] It is also termed ptosis atonia, ptosis adipose and dermatolysis palpebrum . A 21-year-old female presented with laxity of the skin of the upper eyelids for the past 4 months. The problem first manifested at the age of 16 years, when she developed mild fever of 2 days duration followed by bilateral periorbital swelling. This was followed by a gradual increase in the laxity of the skin of the upper eyelids. She underwent cosmetic blepharoplasty in the plastic surgery department of our hospital 3 years ago. Initially, the results were good but, after 1 year, the skin again became lax following eyelid swelling. She was not given any medical treatment and was advised repeat blepharoplasty after stabilization of her condition. Her family history was not contributory and her twin sister did not have similar complaints. Local examination revealed lax wrinkled skin of the upper eyelids with no pigmentary changes [Figure - 1]. The skin at other sites was normal. There was no swelling of the lips or the thyroid region. Her systemic examination was normal. Complete hemogram, liver, renal and thyroid function tests were normal. The exact etiology of blepharochalasis is not known. Most of the cases are sporadic, but autosomal-dominant inheritance has been noted in a few pedigrees. [1] The condition develops insidiously around puberty, characterized by repeated transient attacks of swelling of the eyelids lasting for a few days, followed by laxity, atrophy, wrinkling and pigmentary changes predominantly involving the upper eyelids, although involvement of the lower eyelids [4] and unilateral involvement has been reported. [3] Systemic conditions associated with blepharochalasis are renal agenesis, vertebral abnormalities and congenital heart disease. [5] The eyelid changes cause a lot of cosmetic disfigurement and the affected person looks prematurely aged. About 10% of the cases may have reduplication of the mucous membranes of the upper eyelid, causing apparent thickening of the lids. [1] Three stages are described in the evolution of blepharochalasis. [2] The first is the recurrent angioedema, while the second stage, which is characterized by discolored, flabby and lax skin, is called the stage of atonic ptosis. In the third stage, there is further relaxation of the tissues of the orbital septum, with prolapse of the orbital fat leading to interference of vision. This stage is called ptosis adipose. Most of the cases are reported in the second stage, as in our case. Blepharochalasis can be diagnosed with the help of a proper history and characteristic skin changes of the eyelids. [3] Histopathological examination in the early stages shows mild dermal lymphocytic infiltrate while in the late stages, elastic tissue of the lids is fragmented and decreased. [6] A recent report described immunoglobulin A deposits in the residual elastic fibers, implying the involvement of an autoimmune mechanism. [7] The only effective treatment is correction by plastic surgery after the disease has run its course, otherwise subsequent attacks of lid edema may interfere with the results. [8] Blepharochalasis may be associated with progressive enlargement of the upper lip due to enlargement of the labial salivary glands as well as thyroid swelling in Asher′s syndrome. [8] Ptosis, a common genetic defect, can be distinguished due to the normal appearance of the skin. Generalized cutis laxa and Ehlers-Danlos syndrome may have a similar appearance, but are easily distinguished due to other clinical features. [1] We are reporting this case because of its rare occurrence and its probable relation to fever. References
Copyright 2009 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv09063f1.jpg] |
| |||||||||

{kind=link}