 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
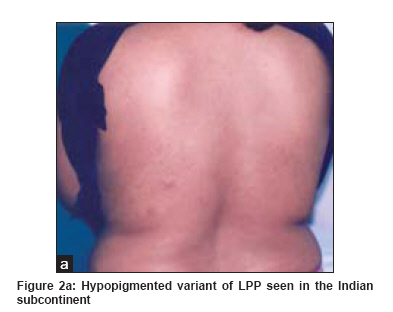
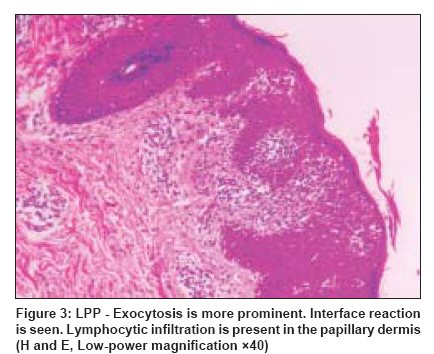
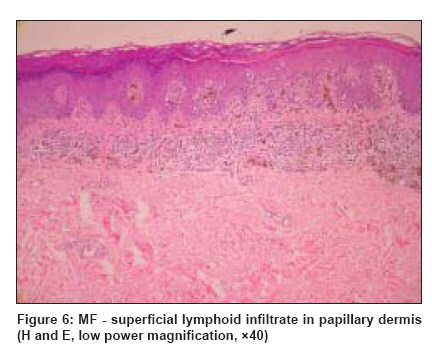
Indian Journal of Dermatology, Venereology and Leprology, Vol. 75, No. 3, May-June, 2009, pp. 229-235 View Point The conundrum of parapsoriasis versus patch stage of mycosis fungoides Sarveswari K.N., Yesudian Patrick Sundaram Medical Foundation, Dr. Rangarajan Memorial Hospital, Chennai, Tamilnadu Code Number: dv09075 PMID: 19439874 Abstract Terminological confusion with benign dermatosis, such as parapsoriasis en plaques, makes it difficult to diagnose mycosis fungoides in the early patch stage. Early diagnosis of mycosis fungoides (MF) is important for deciding on type of therapy, prognosis and for further follow-up. However, until recently, there has been no consensus on criteria that would help in diagnosing the disease early. Some believe that large plaque parapsoriasis (LPP) should be classified with early patch stage of MF and should be treated aggressively. However, there is no firm clinical or laboratory criteria to predict which LPP will progress to MF and we can only discuss about statistical probability. Moreover, long-term outcome analysis of even patch stage of MF is similar to that of control population. We therefore believe that LPP should be considered as a separate entity at least to prevent the patient from being given a frightening diagnosis. We also feel that patients need not be treated with aggressive therapy for LPP and will need only a close follow-up. This article emphasizes the criteria for diagnosing early MF and has highlighted the importance of considering LPP as a distinct benign entity.Keywords: Mycosis fungoides, Parapsoriasis, Small plaque, Large plaque Brocq, in 1902, [1] reviewed the German, French and American literature and reported 10 cases of his own for which he created the term "parapsoriasis," because of their similarity to psoriasis. The common features of these cases were chronicity of disease, absence of symptoms, resistance to available therapy and histologically round cell infiltrate in papillary dermis with spongiosis and parakeratosis. On the basis of mainly clinical manifestations, he differentiated the following subgroups as guttate, plaque and lichenoid. Today, the first subgroup of Brocq′s classification is referred to as pityriasis lichenoides, which has an acute and chronic form. The present terminology of parapsoriasis includes large plaque parapsoriasis (LPP) and small plaque parapsoriasis (SPP). The initiating cause of parapsoriasis is unknown, but the disease probably represents different stages in a continuum of lymphoproliferative disorders, ranging from chronic dermatitis at one end to frank malignancy at the other. Small plaque parapsoriasis, large plaque parapsoriasis and pityriasis lichenoides have all been shown to be monoclonal T cell disorders. These T cells belong to the skin-associated lymphoid tissue (SALT). [2] This has been demonstrated by the T cell receptor gene rearrangement and by the more sensitive polymerase chain reaction (PCR)-based test. A "dominant" clone of lymphocytes had been demonstrated in a few cases of SPP. As this T cell clone did not undergo further mutation that are necessary for the development of mycosis fungoides (MF), SPP is now thought to be a benign disorder with little or no potential to evolve into MF. [3],[4] The lesions of SPP are generally on the upper trunk, 2 to 6 cm in diameter [Figure - 1], rarely up to 20 cm, sometimes with a digitate appearance (digitate dermatosis) and without atrophy or poikiloderma. Histopathology shows non-specific changes (focal spongiosis and psoriasiform or lichenoid dermatitis with exocytosis of small lymphocytes). LPP lesions are larger, more than 6 cm in diameter and localized to buttocks, lower trunk, upper thighs, inner upper arms and inframammary areas (non- sun- exposed areas) and frequently manifest atrophy and/or poikiloderma. Hypopigmented patches are common in the Indian subcontinent [Figure 2a]. Histologically, the pattern of lymphoid infiltration in LPP is similar to SPP [Figure - 3], but the infiltrates often contain lymphocytes with cerebriform nuclei called Lutzner cells similar to that seen in MF. In LPP, the dominant clonal density has been 1% to 10% (in MF 50%). However, it is important to realize that dominant clonality does not equate to clinical malignancy. Although 7.5% to 14% of LPP cases have been reported to progress to MF, most cases run a benign course and remain indolent for many years. In some cases, there has been complete resolution of the disease. Various parameters such as nuclear contour studies, immunohistochemistry, PCR and T cell receptor gene rearrangement studies have all been used to identify the atypical lymphocytes, and thus to predict which LPP will become MF. Even then at best, the diagnosis remains conjectural. Earlier, genotypic analysis of T cell receptor rearrangement study was considered to be the gold standard of all diagnostic tests, holding the unique ability to distinguish between benign and malignant T cell infiltration. Simon et al. , [5] in their study found that of six LPP patients with T cell gene rearrangement studies, only one developed LPP. In others, the disease remained virtually unchanged over follow-up. They thus concluded that even T cell receptor studies could not be relied upon to distinguish between benign and malignant T cell infiltrate. The authors also felt that whether or not LPP is truly early MF, is not the issue; what is important is which patient whether given the diagnosis LPP or early MF (stage Ia) are at risk to develop progressive disease. They concluded that both LPP and early MF do not come under this risk group. LPP has been shown to remain indolent for many years. Close follow-up at least once in six months and repeated biopsies may be needed to rule out progression to malignancy. It can be treated with topical steroids/topical chemotherapeutic agents or with PUVA. [6] Aggressive therapy can be considered as a last resort. Sanchez and Ackerman in 1979 [7] suggested that LPP was synonymous with patch stage of MF. Ackerman later went on to state that even SPP must be considered as patch stage of MF. [8] To consider all parapsoriasis en plaques as early MF simplified a common diagnostic dilemma, but it also raised new problems:
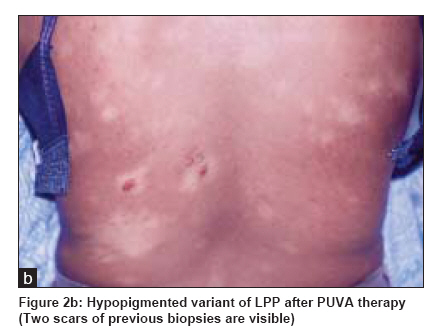
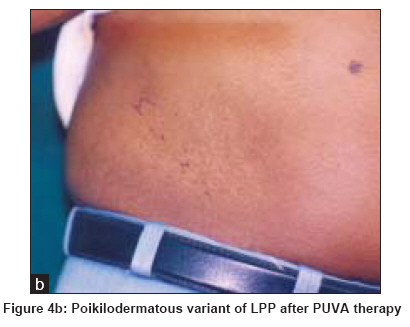
Moreover, including patients with a "benign" course into the mix of patients who have a definite, potentially life-threatening cancer poses added risks for patients: those with "benign" disease are at risk of being treated with aggressive therapy and those with a potential for progressive disease may be deprived of more definitive therapy. We followed up 46 patients with large plaque parapsoriasis (LPP) treated with PUVA between 2000 and 2006. The clinical response was good. Thirty one cases had complete response (>90% clearance), 11 - partial response (50% clearance), 2 - recurrence and 2 - lost to follow-up. The clinical response was seen within 14- 38 treatments (mean 29 treatments). Total UV dose given was 99.5 J-260.5 J (mean, 180 J).Tolerance was good except for mild burning sensation in one patient [Figure 2a] and [Figure 2b] -Hypopigmented variant of LPP - before and after PUVA therapy and [Figure 4a] and [Figure 4b] -Poikilodermatous variant of LPP - before and after PUVA therapy. We concluded the following:
The main difficulty is to differentiate LPP from early MF, as there are no universally accepted minimal criteria for the diagnosis of MF. Recognizing this persistent need to develop standardized diagnostic criteria for early MF, the International Society of Cutaneous Lymphoma (ISCL) has analyzed early MF and have proposed an algorithm for the diagnosis of early "classic" MF that incorporates clinical, histopathologic, molecular biologic and immunopathologic features. [10],[11] The diagnosis of early MF requires a total of four points. Because molecular biologic and immunopathologic criteria represent only one point each, they always require additional clinical and histopathologic criteria to establish the diagnosis of early MF. Conversely, if sufficient clinical and histopathologic criteria are met, then molecular and immunopathologic criteria are not necessary, clinical pathologic correlation thus remaining the gold standard in the diagnosis of MF. [12] Early Diagnosis of MF- Clinical Criteria The ISCL task force for clinical definition of early MF has identified several clinical criteria that are important to recognize classic MF at the initial stage. History Differential diagnosis includes drug eruptions. Withdrawal of an offending drug will eliminate this possibility. Morphology of lesions Another specific clinical feature is poikiloderma [14] (mottled pigmentation, telangiectasia, epidermal atrophy) interspersed with slight infiltration. Persistent poikilodermatous patches on non-sun-exposed areas should be considered as MF until proven otherwise by biopsy. Poikiloderma is not a feature of atopic dermatitis, nummular eczema, psoriasis, lichen planus, pityriasis rosea and SPP, all of which are likely to be clinically confused with MF. Differential diagnosis includes other subtypes of CTCL such as granulomatous slack skin, connective tissue diseases such as dermatomyositis, some genodermatosis and LPP. Number of lesions Differential diagnosis includes nummular eczema, lichen simplex chronicus, erythema chronicum migrans, and tinea corporis. Distribution of lesions ISCL clinical criteria
Early Diagnosis of MF:Histopathologic Criteria To differentiate early MF from other benign dermatosis is an extremely difficult, much debated and yet a crucial issue. Although diagnosis of early stage MF is sometimes inconclusive, careful study may yield the correct diagnosis. [17] To enhance the chance of establishing a histologic diagnosis of MF
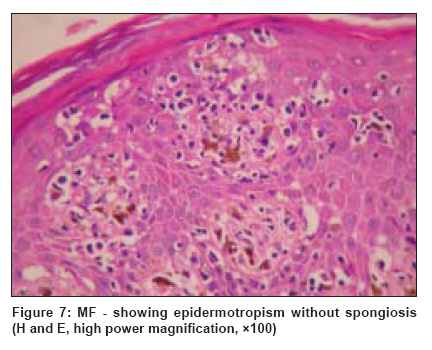
ISCL histopathologic criteria Epidermotropism without spongiosis - 1 point [Figure - 7]. (Differential diagnosis - collagen vascular disease, drug-induced pseudolymphoma) Lymphoid atypia - 1 point [Figure - 7]. (Differential diagnosis-lymphamatoid contact dermatitis, drug-induced pseudolymphoma) The utility of histopathologic criteria is preserved by the interdependence on the other criteria in order to achieve the four points needed to establish the diagnosis of early MF. Caveat The overall clinicopathological features cannot suggest a specific non-MF diagnosis. Early Diagnosis of MF: Ancillary Techniques DNA cytophotometry [18],[19],[20] nuclear morphometry, immunohistochemistry, chromosomal studies and more recently molecular genetic analysis of T cell clonality, have helped in the diagnosis of MF in the early stage. For clonality, PCR-based analysis is more sensitive than Southern blot analysis. It is recommended to use DNA extracted from fresh frozen tissue and PCR-based clonality analysis of T cell receptor gene rearrangements using denaturing gradient gel electrophoresis (PCR/DGGE). [10] The detection of a clonal T cell population by sensitive PCR techniques on frozen specimens that otherwise do not have diagnostic histopathologic features of MF has generated the concepts of "clonal dermatitis" and "abortive/latent lymphoma." [21] Long-term follow-up of patients categorized as having "clonal dermatitis" indicates that progression to overt MF occurs at a rate that may be as much as four times higher than that for large-plaque parapsoriasis defined by clinicopathological criteria alone. Immunohistochemistry [22],[23],[24] can aid in diagnosis of MF. Antigen deficiency must be looked for and MF is generally a CD4 predominant T cell process. CD4/CD8 ratio> 6 and loss of T cell markers (CD7 and sometimes CD5) have been used to support the diagnosis of MF. ISCL molecular biological criteria ISCL immunopathologic criteria
Caveats concerning the algorithm Regardless of any individual feature, if the overall clinicopathologic correlation in a case suggests a specific diagnosis other than MF, then the algorithm ceases to apply (example connective tissue diseases, pseudolymphoma, where history is the key). Recently, cDNA microarray profiling avoids histologic and molecular pitfalls and may be used increasingly in the diagnosis of MF. An early study indicated that a set of six genes accurately differentiated a sample of MF from that of inflammatory disorders. Conclusion When diagnosing early MF, it may be best to err on the conservative side and use strict, rigorous criteria with careful clinical follow-up of borderline cases. A major reason for this is that earlier diagnosis and treatment is not necessarily beneficial to patients. Studies have revealed that PUVA treatment of mycosis fungoides patients (stages Ia to IIa), although effective in achieving a complete response, about 50% of patients developed a relapse after a median of 33 months and one-thirds of patients developed photodamage and skin cancer. [27] Maintenance phototherapy is not warranted. Survival did not worsen in patients who had relapse. [28] Another study compared topical treatment of mycosis fungoides with electron-beam radiation and chemotherapy and found no difference in prognosis between the topical versus systemic treatments, although increased morbidity was associated with systemic treatment. [29] We have tried to emphasize the point that in developing countries, where only clinicopathological correlation is possible in the majority of cases and hence diagnosis of MF is conjectural, we believe that the diagnosis of MF should not be offered to the patient. This can lead to unnecessary expensive aggressive therapy and may also cause great distress and even suicidal thoughts in the patient. Patients are only concerned about the cosmetic disfigurement caused by hypo- or hyperpigmented patches and are not worried about semantics, whether we call it as large plaque parapsoriasis or patch stage MF. As the treatment of both the disease is the same, for example, PUVA, [28] and as one cannot be certain which of the early mycosis fungoides will go into the tumor stage, it makes sense to use a "benign" term such as large plaque parapsoriasis rather than the "malignant" term MF. It is more compassionate for the patient whatever the demerits of the term parapsoriasis may be. That is our only argument for holding on to the "retrogressive" terminology of parapsoriasis. It is essential though to have a close follow-up of these patients. It is this aspect that has to be emphasized. Acknowledgment Dr. Jessy Thomas - Pathologist, Dr. A. Bridgette Akila - Epidemiologist, Ms. J. Shylaja - Secretarial Assistance.References
Copyright 2009 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv09075f1.jpg] [dv09075f7.jpg] [dv09075f4b.jpg] [dv09075f2b.jpg] [dv09075f3.jpg] [dv09075f4a.jpg] [dv09075f2a.jpg] [dv09075f5.jpg] [dv09075f6.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}