 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
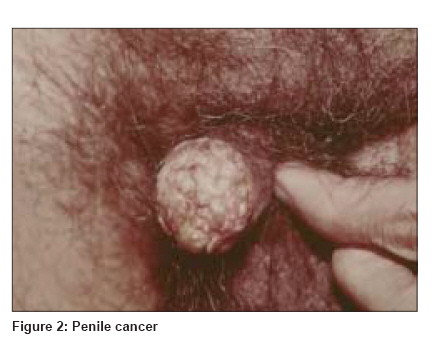
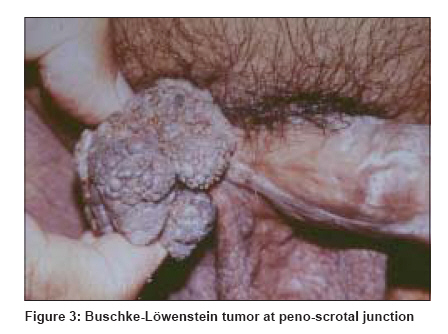
Indian Journal of Dermatology, Venereology and Leprology, Vol. 75, No. 3, May-June, 2009, pp. 236-244 Review Article Human papillomavirus and genital cancer Rapose Alwyn Division of Infectious Diseases, Department of Internal Medicine, University of Texas Medical Branch, Galveston, Texas Code Number: dv09076 PMID: 19439875 Abstract Human papillomavirus (HPV) is one of the most common sexually transmitted infections world-wide. Low-risk HPV-types are associated with genital warts. Persistent infection with high-risk HPV-types is associated with genital cancers. Smoking and HIV infection have consistently been associated with longer duration of HPV infection and risk for genital cancer. There is an increasing incidence of anal cancers, and a close association with HPV infection has been demonstrated. Receptive anal sex and HIV-positive status are associated with a high risk for anal cancer. Two HPV vaccines are now available and offer protection from infection by the HPV-types included in the vaccine. This benefit is maximally seen in young women who were uninfected prior to vaccination.Keywords: Anal cancer, Cervical cancer, HPV vaccine, Human papillomavirus Introduction Human papillomavirus (HPV) is a highly diverse group of viruses, ubiquitous in nature, with world-wide distribution. HPV has been detected from apparently normal skin [1] and appears to have a highly variable latent period before detectable pathology. HPV is associated with lesions ranging from benign cutaneous warts, to recurrent laryngeal papillomatosis, [2] to malignancies like cervical cancers. It is the most commonly occurring sexually transmitted infection in the United States and the United Kingdom. "Low- risk" HPV-types 6 and 11 are the most common HPV associated with genital warts and most cases of recurrent respiratory papillomatosis. "High-risk" HPV- types 16 and 18 are HPV most commonly associated with cervical dysplasia. HIV- infected females have a higher risk - compared to HIV uninfected women - to progress from benign HPV genital infection to cervical dysplasia and cervical cancer, and cervical cancer is included in the definition of AIDS. There has been an increasing incidence of anal cancer in the Unites States, and HPV has been implicated as an etiologic agent. [3] Highest risk is seen in HIV-positive persons and male homosexuals. This review will focus on the association between HPV infection and genital cancers with emphasis on cervical cancers in females and anal cancer in both males and females. Two HPV vaccines are now available and data on studies with these vaccines will also be reviewed.Classification and Nomenclature[4] HPV in Women Knowledge about the relationship of HPV to cervical cancer is low even in the United States [9],[10] and the United Kingdom. [11] Most women rely on their primary care physician for this information. [12] Unfortunately physicians themselves may be lacking in awareness. [13] Recommendations regarding early detection and prevention of cervical cancer are discussed in detail in Guidelines of The U.S. Preventive Services Task Force -USPSTF and can be accessed at: http://www.ahrq.gov/clinic/uspstf/uspscerv.htm . Guidelines of the American Cancer Society can be found at http://caonline.amcancersoc.org/cgi/content/short/52/6/342 . Although cervical cancer screening with Papanicolaou (Pap) smear has allowed early detection and treatment of cervical pre-malignant lesions, resulting in a significant reduction of cervical cancer and its related mortality, 11,150 new cases of cervical cancer, associated with 3670 deaths were reported in the U.S. in 2007. [14] There were also an additional 5630 new cases of other vulvo-vaginal cancers. A significant increase in invasive vulvar cancer was also reported in a German study, with a majority of the women < 50 years being HPV-positive. [15] In India, there are more than 130,000 reported new cases of cervical cancer every year. [7] Traditional screening with Pap smear has been difficult to implement in India and Patro [16] has reviewed prevention strategies including visual inspection methods. Persistent HPV infection has now been recognized as a "necessary" etiologic factor for cervical cancer, and is also closely associated with less invasive forms of cervical intraepithelial lesions. A number of studies have tried to define the HPV-types and the incidence, prevalence, duration and rate of clearance of HPV infection in various populations. The results vary depending on the population evaluated, the mean age (prevalence is higher in a younger population), the site of collection of samples (cervical swabs v/s cervico-vaginal lavage (CVL) v/s additional perineal skin swabs) and most importantly- the laboratory tests used to detect and type the HPV. [17] A meta-analysis of nine studies from India by Bhatla et al. , [18] revealed an overall HPV prevalence of 12% in women with normal cytology and 94.6% in women with invasive cervical cancer. HPV-16 and 45 were more prevalent in patients with cervical cancer in North India, compared to HPV- 35, which was the more prevalent HPV in patients with cervical cancer in South India. In a recent report from the All India Institute of Medical Sciences, HPV- 16 was seen in 74.3% cases with high grade squamous epithelial lesions. [19] The other HPV-types associated with high grade disease included HPV-18, 33, 35, 39 and 56. In a report by Insinga et al. , [20] prevalence for HPV-16 and18 was 6.8% and 2.6% respectively. The combined prevalence of either HPV-6, 11, 16 or 18 was 12.1%. The calculated incidence was 5.4 per 100-person-years for HPV-16, and 2.1 per 100-person-years for HPV-18. The study population only involved young U.S. women aged 16 - 23 years, and they were evaluated only for HPV-types 6, 11, 16 and 18. Winer et al. , evaluated young college women in Washington State, U.S. testing 18 different HPV-types. They detected a prevalence of 19.7% for any HPV-type. [21] Limitations of this study, however, were that only 20% of the eligible women agreed to enroll and the prevalence of individual HPV-types was not reported. A 24-month cumulative incidence of new infections was reported as highest for HPV-16 (10.4%), followed by HPV-6 (7.5%). Risk factors for acquiring a new HPV infection included sex with a new person in the previous 5-8 months, smoking and use of oral contraceptives. "Always using condoms" did not provide protection according to this study. Interestingly, only 3 samples (0.39%) collected during 757 visits from virgins were positive for HPV-16. In a large population- based study in Columbia involving women aged 18-85 years, the prevalence of HPV infection was 15%, with HPV-16 being the most frequently detected type (16% of all infections). [22] Higher prevalence figures can be expected because probes to detect 37 different HPV-types were used. High percentages were also noted in the HIV Epidemiology Research Study (HERS) cohort study. [23] These were females at risk for HIV infection. The prevalence of HPV infection was 55% in HIV-positive females and 26% in those who were HIV-negative. A wide spectrum of HPV-types were evaluated and among those who were HIV-positive, HPV-53 - a non-high-risk type - was the most common (8.4%), while HPV-83 - also a non-high-risk type (7.1%)-was most common in the HIV-negative women. Overall, HIV-positive women had a higher prevalence of HPV infection. HIV-positive women also have a higher incidence of HPV related cervical dysplasia, and have multiple HPV types simultaneously. [24],[25],[26] The HPV- types most commonly seen in HIV-positive women were 56, 53, 16, 58, 52, MM7, MM8 and 33 in one study of women attending an AIDS clinic in New York. [24] HPV- 56 and 53 were most commonly associated with low grade squamous intraepithelial lesions, and HPV- 52 and 58 were associated with high grade squamous intraepithelial lesions in this population (cervical brush and CVL specimens were evaluated). Different results were obtained by another group from South Africa, [26] who found that HPV-16 was the most prevalent in HIV- positive women with abnormal cervical cytology (only endocervical samples were evaluated). The differences may be partly explained by differences in sampling techniques. It is believed that although HPV infection is common, progression to neoplasia is less frequent because the majority of females with genital HPV infection clear the virus on their own. In terms of duration and rate of clearance of HPV infection, once again the studies differ in their results. In a study by Giuliano et al. , 100% of the cohort members who were positive for HPV-16 at baseline, were negative at 12 months, with an estimated median time to clearance being 9.8 months for oncogenic HPV- types and 4.3 months for non-oncogenic types. [27] The estimated duration for all HPV infections in the HERS cohort was 0.8 years in women who were HIV- positive and 0.6 years for those who were HIV-negative. [23] However, longer duration of infection was observed in other studies. In the population evaluated by Insinga and colleagues, the reported duration of infection was 18.2 months and 16.4 months for HPV-16 and HPV-18 infection respectively. [20] In the Columbian cohort study, less than 80% HPV infections had cleared by 1 year and around 92% had cleared the infection by 5 years. [22] Being a current smoker may prove to be an independent predictor of longer persistence. HIV-positive females also have higher persistence of HPV infection. [23] High- risk types are associated with higher persistence, [27] with HPV- 16 having the longest persistence. [20],[22],[23] Host factors including number of sexual partners and concomitant sexually transmitted infections may also play a role in HPV persistence. The incidence of anal cancer in both males and females has increased over the last decade with more than 4600 cases reported in the United States in the year 2007. [14] HPV has been implicated as an etiologic agent. [3],[28] Goodman et al. , evaluated anal cancer in females and the association with HPV and concluded that risk factors mirror those for HPV-related cervical cancer. [29] Receptive anal intercourse is an additional risk factor, and the risk appears to be higher in HIV-positive persons. [30],[31] There is also some risk in persons denying history of anal intercourse, [32] but this data has limitations as it is based on participants′ self- reporting behaviors. HPV in Men Genital HPV infection in men may be asymptomatic or they may present with penile and perineal warts [Figure - 1] In a study of males attending vasectomy clinics in Mexico (i.e. without symptoms of genital warts), the prevalence of any HPV was 8.7%. [33] In this group the most common type was HPV-59 (1.5%), with HPV-16 coming in fourth (0.8%). In an attempt to study the cumulative incidence of HPV infection in an apparently healthy sexually active male cohort, Partridge et al. , [34] evaluated new recruits to the University of Washington in Seattle. In 468 sexually active males less than 20 years of age, the cumulative incidence of HPV at 24 months was calculated to be around 64%. Also in this group the most common HPV-type was 84 (low risk type) (23.3%), with HPV-16 coming in as second (19.5%) and HPV-18 a distant ninth (7.5%). However, this data does not provide any idea of the prevalence of HPV in the overall community of young male college students as only 3.7% of the new recruits were enrolled in the study. Interestingly, there was a cumulative incidence of 32% HPV infection under the fingernails of the hands. As can be expected, prevalence of genital HPV infection is higher among males attending STD clinics. In one U.S study of this population, the prevalence of any HPV on the penis was close to 30% [35] and the most common HPV-type was non-oncogenic HPV-6 (3.85%). HPV- 16 came in fourth (2.3%) behind other non-oncogenic HPV 53 and 84. In a study of a similar population from Denmark, [36] higher rates (45%) with HPV-16 being the most prevalent (15% of all positives) were reported. In this study, specimens included swabs from the penis as well as perineum. Risk factors for genital HPV infection in males include life time number of sexual partners [33],[36] and smoking. [33],[34] The role of circumcision in protection against HPV infection remains inconclusive with some studies indicating a benefit. [33],[36],[37] But this was not seen in other studies. [34],[38],[39] 1280 cases of penile cancers [Figure - 2] were reported in the U.S. in 2007. [14] The association with HPV infection (50% [40] 77% [41] ) is less consistent compared to that with cervical cancer. HPV-types 6, 11 and 16 are consistently found in giant warts and Buschke- Lφwenstein tumors [Figure - 3] of the penis and perianal region. A high proportion of these are associated with squamous cell carcinomas. Increasing attention is now being focused on the association of HPV infection and anal cancers in males. Fifty asymptomatic male partners of females with HPV infection were evaluated in a study by Nicolau and colleagues. [42] 76% were HPV- DNA-positive, and 8% had HPV in the anus. Prevalence of anal HPV infection was higher in males with HIV-infection (46% in HIV-positive men who denied having anal sex in a study by Piketty et al. [32] ) and even higher in men who have sex with men (85% in HIV-positive men in the study by Piketty et al. [32] and 83% in HIV-positive men in a study by Sirera et al. [43] ). The most prevalent type was HPV-16 in these two studies. In contrast, Nyitray et al ., [44] evaluated 253 asymptomatic heterosexual men from two U.S. cities for anal HPV infection and found a prevalence of 24.8%, the most common type being HPV-68, a non-oncogenic type. Apparently their only risk factor was sex with more than one female. The prevalence thus varies depending on the population of patients evaluated, the site of collection of samples [45] and the test used to detect and type the HPV. Perianal warts in males were reported to be associated with a high frequency of anal intraepithelial neoplasia, more so in HIV-positive patients (up to 52%). [46] However, this data has to be interpreted with caution as lesions evaluated by histopathology were large and possibly treated previously with therapies known to alter cell morphology, details of which were not presented in the article. Condoms have not shown a protective benefit for females against acquiring HPV infection. [21],[47] In terms of protecting males from acquiring HPV infection via vaginal intercourse, the data has been conflicting. Some studies claimed a benefit (e.g. Vaccarella et al ., [33] 13% of the study population reported condom use- and Baldwin et al. , [37] only 15% participants reported condom use "every time", while nearly 40% reported "never" using condoms in the 3 months prior to the interview; swabs were obtained only from the penis, and adjacent perineum was not sampled) while other studies have demonstrated no significant benefit. [36],[48] This is possibly related to the fact that condoms cannot protect skin beyond that immediately covered [47],[49] and that HPV is also found on the pubis, male scrotum [Figure - 3] and female vulva. There is also a high rate (20-30%) of condom breakage and slippage. [50],[51] In terms of protection from HPV acquired via anal intercourse between males, the data is even more concerning with one study reporting very low (42%) condom use among male homosexuals practicing anal intercourse. [52] A panel of experts (including those from the Center for Disease Control and Prevention and the National Institutes of Health) reviewing published literature concluded "there was no epidemiological evidence that condom use reduced the risk for HPV infection". [53]HPV in the Oral Cavity and Relationship to Genital HPV There is an association between oral HPV infection and oral cancers. HPV-16 and 18 are the most prevalent types associated with cancers in the regions of the head and neck. [54],[55] Giraldo et al ., detected a higher prevalence of oral HPV in females who had genital HPV infection, and vice-versa. [56] However data on HPV-types was not presented. Fakhry et al ., [25] evaluated HPV-types in the oral cavity and the genitals of the same patients. 93.7% patients had no concordance between the HPV-types in the oral cavity and the cervical samples. Marais et al ., also found no concordance between oral and cervical HPV types. [26]The HPV Vaccines A failure to clear HPV from infected cells leading to persistent infection has been related to defective host immune response as well as possibly a viral immune evasion mechanism. [57] To improve host immune response to clear invading HPV, two "L1 virus-like- particle" HPV vaccines are now available, a quadrivalent vaccine (Gardasil ® ) involving HPV-types 6, 11, 16 and 18 [58] (licensed for use in the United States in June 2006) and a bivalent vaccine (Cervarix ® ) involving the two most prevalent HPV oncotypes 16 and 18 [8] (approved for use in Australia and Europe). They are administered as 3 intramuscular doses, first dose on day 1, second dose 1 month later and third dose at 6 months. These vaccines have been demonstrated to confer protection against the two most common high- risk HPV associated with cervical cancer in young women who were uninfected by these two types at the time of vaccination. Olsson et al ., [59] evaluated the anti- HPV antibody response in vaccinated persons up to three years after initial vaccination. They demonstrated a decline in antibody levels post-vaccination, but levels reached a plateau at 2 years and remained at that level up to 5 years. When 114 of these subjects received an extra dose of the vaccine 5 years after the primary series, there was evidence of an increase in the antibody titre. This was higher than the titre obtained 1 month after completion of the primary series, indicating that vaccination may induce "immune memory". In a combined analysis of three randomized clinical studies, the quadrivalent vaccine was evaluated in 18,174 women aged 16-26 years. [60] Participants were followed-up for a mean period of three years for the development of high grade vaginal and vulvar intraepithelial neoplasia. The vaccine conferred 100% protection against HPV- types 16/18-associated high grade vaginal and vulvar intraepithelial neoplasia in those who completed three doses and who were negative for HPV-16 and 18 one month after the third dose. In other words, the vaccine was most effective in preventing high grade neoplasias associated with the HPV-types included in the vaccine (HPV-16 and 18) and only in females who were naοve for HPV-16 and 18 infection prior to and up to 1 month of vaccination. Unfortunately it was less than 50% effective in preventing all-type high grade vaginal and vulvar intraepithelial neoplasias. Similar efficacy data concerning the prevention of cervical disease were demonstrated for the bivalent vaccine.[8] However, the number of patients included was much smaller, only cervical samples were evaluated, PCR testing was done only for HPV-16, 18 and related HPV types, and all-type high grade vaginal and vulvar intraepithelial neoplasias were not evaluated. Similar drawbacks are inherent even in more recent efficacy studies of these vaccines, in that while there may be a demonstrable protection against vaccine-type HPV related neoplasias in those naοve to these infections, overall reduction of cervical and anogenital diseases was only around 20-35%. [61] Hence recommendations to vaccinate without prior screening for HPV status [62] and calls for wide-scale adoption of HPV vaccination need to be tempered by the fact that up to 35% of cervical cancers may be caused by other HPV-types, though cross-protection to species-related HPV-types has been noted. [8] Also, data on prevalence of HPV-types is lacking from the majority of countries with high incidence of genital warts, vulvar neoplasias and cervical cancer, and the predominant HPV-types may actually be different. [63] In a recent study from Canada, HPV-31 was almost four times more prevalent than HPV-18 in women with grade 2 cervical intraepithelial neoplasia. [64] HPV-52 and 58 were more prevalent than HPV-18 in a study from Taiwan. [65] In a study in Costa Rica of over 2000 patients with previous HPV infection, there was no evidence of benefits in terms of rate of clearance of vaccine-type HPV infection and the authors suggested that it was unlikely that vaccination could have a beneficial impact on rate of lesion progression to malignancy. [66] Also, natural infection with HPV has an unknown latent period prior to evidence of genital warts and possibly even longer duration of persistent infection is required for development of epithelial neoplasias. Data regarding such long-term benefits of vaccination is currently lacking. Whether HPV-types not included in the vaccine will fill the space created by suppression of vaccine-types - as is beginning to be observed in pneumococcal infection - remains to be seen. The role of the vaccine in males in the prevention of penile and anal cancer is unclear so far. Similarly, vaccination of HIV-positive women who are a high risk group for genital cancer needs to be evaluated. Studies attempting to address these questions are ongoing.Conclusions HPV is one of the most common sexually transmitted infections world-wide. Prevalence is higher among smokers, those with multiple sexual partners, and HIV-positive persons. Data on incidence and prevalence need to be interpreted in light of the population being evaluated, the method and site of collection of specimens and most importantly the laboratory tests used to detect and type the HPV. Rates of spontaneous clearance of genital HPV infection are high. Persistence of high-risk-types like HPV-16 and 18 is associated with dyspalsia and malignancy in males and females. HIV-positive persons have a higher risk of having multiple HPV-types simultaneously; have more persistent HPV infection and a higher risk for cervical dysplasia. There is an increasing incidence of anal cancers in both females and males. HIV infection and receptive anal intercourse markedly increase risk for anal HPV infection and anal cancer. Studies have revealed anal HPV infection even in those without clinical lesions and without a history of receptive anal intercourse. Condom use has not been demonstrated to provide adequate protection from acquiring HPV infection in females, and reports of benefits in males are not consistent. The HPV vaccines appear to provide protection from HPV infection up to 3 years in studies in the U.S., Europe and a few other countries. This protection is nearly 100% for the HPV-types included in the vaccine, in addition to cross-protection to a certain number of species-related HPV-types, and in young women who did not have infection at the time of vaccination. The vaccines have been less successful in reducing all-type cervical dysplasia and anogenital disease, and follow-up studies are in progress.References
Copyright 2009 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv09076f2.jpg] [dv09076f1.jpg] [dv09076f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}