 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Dermatology, Venereology and Leprology, Vol. 75, No. 3, May-June, 2009, pp. 272-278 Original Article Profile of acne vulgaris-A hospital-based study from South India Adityan Balaji, Thappa Devinder Mohan Department of Dermatology and STD, Jawaharlal Institute of Postgraduate Medical Education and Research (JIPMER), Pondicherry Code Number: dv09081 PMID: 19439880 Abstract Background: Acne vulgaris is believed to be the most common disease of the skin. There is no Indian study on the profile of acne vulgaris, markers of severe forms of acne vulgaris and a possible correlation between acne vulgaris and markers of androgenicity in females.Aim: To study the profile of acne vulgaris, its seasonal variation, relationship with smoking and possible correlation between acne vulgaris and markers of androgenicity in females. Methods: The study was conducted between August 2006 and June 2008. All patients with acne vulgaris who consented to participate in the study were included. The parameters evaluated included age, gender, age of onset, duration of lesions, site of lesions, grade, relation with menstrual cycle, markers of androgenicity, number of acne lesions such as comedones, papules pustules and nodules, number and site of post-acne scarring, post-acne hyperpigmentation, seasonal variation and history of smoking. Results: A total of 309 patients with acne vulgaris were included in the study. The frequency of acne vulgaris in our study was 1.068%. Mean age of the study group was 19.78 years. Male to female ratio was 1.25:1. The most common age group involved was 16 to 20 years (59.8%). Mean age of onset was 15.97 years. Face was involved in all the patients, followed by back (28.2%), chest (20.1%), neck (9.4%) and arms (10%). In the older age groups, women were more likely to report having acne vulgaris than men ( P = 0.01). The closed comedones outnumbered open comedones by a factor of 4.9:1. A total of 186 patients (60.2%) had grade 1 acne vulgaris, 85 (27.5%) had grade 2 acne, 8 (2.6%) had grade 3 acne and 30 (9.7%) had grade 4 acne vulgaris. There was a higher incidence of scarring (39.5%) and post-acne hyperpigmentation (24.6%) in our study. In female patients, 57.7% had premenstrual flare and 12.4% had cutaneous markers of androgenicity. There was no association between severity of acne vulgaris and other markers of androgenicity ( P = 0.108). Seborrheic dermatitis (21.35%) was the most common disease associated. Seasonal variation was observed only in 80 patients (25.9%); 71 patients (23%) exacerbated in summer and 9 patients (2.9%) in winter. Smokers had more severe grade of acne vulgaris compared to nonsmokers ( P = 0.001). Conclusion: This study brings out the clinical profile of acne vulgaris in a tertiary care hospital in South India. Keywords: Acne vulgaris, Comedones, Post-acne scarring, Post-acne pigmentation, Androgenicity Introduction Acne vulgaris is a chronic inflammatory disease of the pilosebaceous units. [1] It is believed to be the most common disease of the skin. [2],[3] The condition usually starts in adolescence, peaks at the ages of 14 to 19 years and frequently resolves by mid-twenties. Acne vulgaris develops earlier in females than in males, which may reflect the earlier onset of puberty in females. The most severe forms of acne vulgaris occur more frequently in males, but the disease tends to be more persistent in females. [1] Severity of the disease varies markedly from one individual to the other depending upon the interplay of various factors involved in the development of acne vulgaris. Grading systems based on the clinical appearance of lesions as well as "lesion counting" are useful in assessing the severity of acne vulgaris. Although very common, the disease can cause significant emotional distress and physical scarring if left untreated. To the best of our knowledge, there is no Indian study on the profile of acne vulgaris, its seasonal variation, relationship with smoking and possible correlation between it and markers of androgenicity in females. Our study was undertaken to address these issues. Methods This study was conducted between August 2006 and June 2008. All patients with acne vulgaris attending our outpatient department (OPD) who consented to participate in the study were included. Patients with acne vulgaris not willing to participate in the study and patients with drug-induced and other acneiform eruptions were excluded. The parameters evaluated include age, gender, age of onset, duration of lesions, site of lesions, grade, relation to menstrual cycle, markers of androgenicity, number of acne lesions such as comedones, papules pustules and nodules, number and site of post-acne scarring, post-acne hyperpigmentation, seasonal variation and history of smoking. Acne vulgaris was graded using a simple grading system taking into account the predominant lesion to grade acne, which classifies acne vulgaris into four grades. [4]
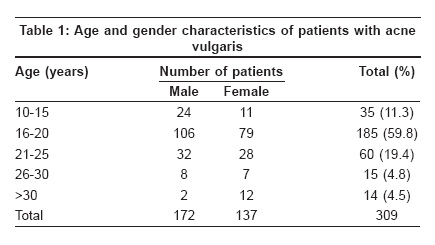
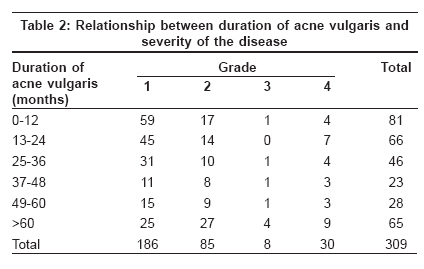
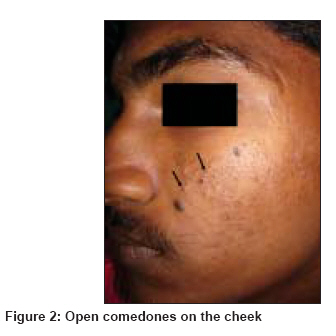
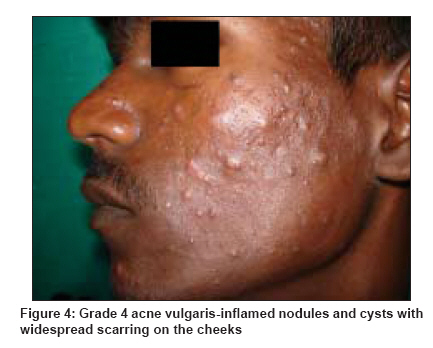
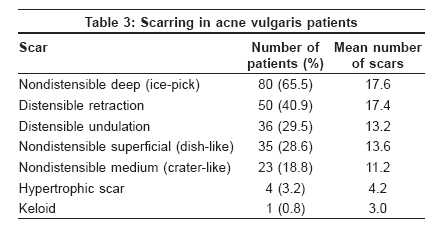
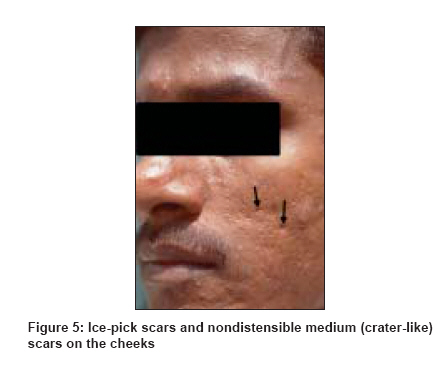
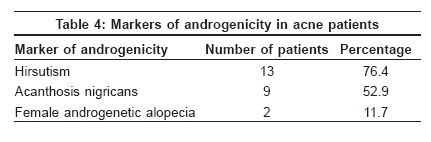
Results Of the 28,917 new patients who attended the dermatology OPD during the study period, 309 patients had acne vulgaris and the frequency was 1.068%. Of the 309 patients, 137 (44.3%) were females and 172 (55.7%) were males. Male to female ratio was 1.25:1. The age of the patients varied from 13 to 45 years with the mean of 19.78 years (SD ± 4.94). The most common age groups to be involved in acne vulgaris were 16-20 years (185 cases, 59.8%) and 21-25 years (60 cases, 19.4 %). [Table - 1] shows age and gender characteristics of the patients with acne vulgaris. It was found that patients aged 20 years or older (89 vs. 220) are more likely to have severe grade of acne vulgaris ( P = 0.011). It was also found that male patients had more severe acne vulgaris ( P < 0.0001) (30 males vs. 6 females had grade 4 acne vulgaris). Mean duration of acne vulgaris was 45.55 months and the range was 1 month to 25 years. Patients with longer duration of the disease had more severe acne vulgaris ( P = 0.022) [Table - 2]. Mean age of onset of patients in this study was 15.9 years (SD ± 3.004) (range, 10-33 years). The mean age of onset in male patients (15.9 ± 2.33 years) was earlier compared to female patients (16.05 ± 3.68 years). However, this was not statistically significant ( P = 0.112). A majority of the patients were college students (33.3%) or school students (33%). Face was involved in all the patients with acne vulgaris. However, face alone was involved in 202 (65.4%). This was followed by the involvement of the back (28.2%), chest (20.1%), neck (9.4%) and arms (10%). The most common type of lesion in this study was closed comedones, present in all patients [Figure - 1] (mean count = 6.67; range = 0-118 at various sites). Open comedones [Figure - 2] were the second most common type of lesion of acne vulgaris (mean count = 1.36; range = 0-85 at various sites) followed by papules (mean count = 1.13;range = 0-30 at various sites), pustules (mean count = 0.17; range = 0-30 at various sites) and nodulocysts (mean count = 0.11; range = 0-18 at various sites). The mean number of noninflammatory lesions was 4.02 and that of inflammatory lesions was 0.47. The ratio of noninflammatory to inflammatory lesions was 8.55:1. The closed comedones outnumbered open comedones by a factor of 4.9:1. A total of 186 patients (60.2%) had grade 1 acne vulgaris, and 85 (27.5%) had grade 2 acne. Grade 3 acne vulgaris was diagnosed in 8 patients (2.6%) [Figure - 3] and grade 4 acne vulgaris in 30 patients (9.7%) [Figure - 4]. Post-acne scarring was seen in 122 patients (39.5%). Cheeks were the most common site of post-acne scarring, being involved in all the 122 patients. Nondistensible deep scars (ice-pick scars) were the most common type of scars (65.57%) [Table - 3],[Figure - 5]. Patients with longer duration of the disease are more likely to have post-acne scarring (56.03% in duration> 3 years vs. 29.5% in duration < 3 years; P < 0.001). Post-acne hyperpigmentation was observed in 76 patients (24.6%). Fourteen female patients (10.2%) gave a history of irregular menstrual periods. Seventy-nine female patients (57.7%) gave a history of premenstrual flare. Seventeen patients (12.4%) had some marker of androgenicity. The most common marker of androgenicity observed was hirsutism (76.4%) [Table - 4]. There was no association between severity of acne vulgaris and other markers of androgenicity ( P = 0.108). Seborrheic dermatitis was the most common disease associated with acne vulgaris (21.35%). Seasonal variation was observed only in 80 patients (25.9%); 71 patients (23%) exacerbated in summer and 9 patients (2.9%) in winter. In 39 patients (12.6%), duration of disease was less than 12 months; hence, seasonal variation could not be determined. Only 10 patients (3.2%) were smokers. Men who were smokers had more severe grade of acne vulgaris compared to nonsmokers (50% smokers vs. 8.36% nonsmokers had grade 4 acne vulgaris; P = 0.001). Discussion Acne vulgaris is a chronic condition that is virtually universal in adolescence. An individual is more likely to develop acne than any other disease. [1] Hospital-based studies done on acne vulgaris in Asian population have shown that acne vulgaris constitutes 11.2% and 19.6% of the total new patients attending their hospitals. [5],[6] A survey of Australian private dermatology practices reported that of 3197 new diagnoses, 320 (10%) patients were for acne. [7] In our study, acne vulgaris accounted for 1.06% of the total number of new patients examined in our center. Frequency of acne vulgaris in our study was low probably due to a low prevalence of acne vulgaris among South Indian population. Al-Ameer and Al-Akloby, [5] in their study of 225 patients with acne vulgaris observed that the age at presentation was 19.2 ± 3.0 years for males and 18.4 ± 4.2 years for females. Kane et al . [8] noted that the mean age of presentation of their patients was 25.58 years. The mean age of patients in our study population was 19.78 years (SD ± 4.94). Unlike teenage acne, where males tend to show the most severe forms of the disease, adult acne mainly affects females. [1],[9],[10] In our study also, in the older age group, women were more affected by acne vulgaris than men ( P = 0.01). In accordance with earlier studies, [11],[12] it was found in our study also that severe acne occurred commonly in patients of older age group. Another interesting observation made in our study was that male patients had more severe acne vulgaris as recorded in other studies. [11],[13] Acne vulgaris develops earlier in females than in males. [1],[2],[5],[11],[13],[14] The earlier onset of clinical acne in girls than boys is presumably related to their earlier puberty. However, in our study, there was no significant difference regarding the age of onset of acne vulgaris among both sexes. Acne vulgaris occurs in sites, which are rich in pilosebaceous units. It was noticed in our study that face was the theater of action in all the patients with acne vulgaris (100%), back was involved in 28.2%, chest was involved in 20.1%, neck was involved in 9.4% and arms were involved in 10%. These observations are in accordance with data from earlier literature. [1],[15],[16] Acne vulgaris is a polymorphic disease. [1] The primary and the pathognomonic lesion of acne vulgaris is a comedone, which may be open or closed. [15] Kilkenny et al . [11] and Cunliffe et al . [17] reported that comedones were the most common type of lesion. It is known that the closed comedones are usually present in much greater numbers than open comedones. [18] The most common type of lesion in our group of acne patients was closed comedones. In our study, we graded the severity of acne vulgaris, using a simple and quick system of classification using a four-grade system. [4] Although our study is a hospital-based study, patients with grade 1 (predominantly comedonal) acne vulgaris outnumbered patients with more severe inflammatory forms of the disease. Similar finding was noticed by Kane et al. [8] in their study. Kane et al. [8] noticed that 40.2% of their 93 patients with acne vulgaris had post-acne scarring. Lower incidence of post-acne scarring in acne vulgaris patients has been recorded in other studies. Kilkenny et al. [11] reported 25% of the 615 patients with post-acne scarring. Taylor et al. [19] also noted 5.9% of their patients with post-acne scarring. Post-acne scarring was noticed in 39.5% of our acne patients. The relatively high incidence of post-acne scarring may be a phenomenon in the South Indian race. We also observed that patients with longer duration of the disease were more likely to have post-acne scarring. This is an expected finding, which is also reported in earlier studies. [10],[20] The ice-pick scars were the most common type of post-acne scars, noticed in 65.57% of the patients with post-acne scarring. The findings in our study were in accordance with those of Layton et al . [20] Postinflammatory hyperpigmentation is a common complication of acne vulgaris, particularly in pigmented skin. [1] Kane et al. , [8] noted that 67.7% of their patients had post-acne pigmentation. Similarly, Yeung et al. , [21] observed 552 adolescent patients with acne vulgaris, of which 52.6% had hyperpigmentation. Taylor et al. [19] noticed 52.6% of their patients with postinflammatory hyperpigmentation. Post-acne hyperpigmentation was observed in 76 patients (24.6%) in our study. The incidence of postinflammatory hyperpigmentation in our study was lower compared to that in earlier studies. The premenstrual acne flares is well recognized. The pilosebaceous duct becomes smaller between days 15 and 20 of the menstrual cycle and the blockage leads to premenstrual acne. However, the mechanism for this blockage is not known. [22] Stoll et al. [23] found an overall 44% prevalence of premenstrual flare. Khanna and Pandhi . [24] noticed a mean reduction in the noninflammatory and inflammatory lesions count during the postmenstrual period. Premenstrual flare was noticed in 57.7% of the 137 female patients in our study. The incidence of hirsutism and irregular menses observed in earlier studies [25],[26],[27] varied between 0% to 21% and 15.5% to 48%, respectively. The corresponding figures in our study were 9.48% and 10.2%, respectively. Sheehan-Dare et al. [28] and Cibula et al. [26] concluded that there is no correlation between acne severity and clinical markers of androgenicity in women. Although these studies have shown no correlation between acne severity and markers of androgenicity, previous studies including one done by Reingold and Rosenfield . [29] have found an association between acne, hirsutes and menstrual disturbance. In our study, we observed no association between severity of acne vulgaris and clinical markers of androgenicity. Both acne vulgaris and seborrheic dermatitis have predilection for the seborrheic areas of the body such as face, ears, scalp and upper part of the trunk. Moreover, it is well known that seborrhea plays a central role in the pathogenesis of both the diseases. In seborrheic dermatitis as well as in acne vulgaris, the lipid composition of sebum is characterized by a high triglyceride level. [30] In a Spanish study involving 2159 patients with seborrheic dermatitis, it was found that acne vulgaris was the most common concomitant disease seen in 35% of the subjects. [31] Seborrheic dermatitis was the most common disease associated with acne vulgaris in our study. The relationship between smoking and acne vulgaris is controversial. Mills et al. [32] and Rombouts et al. [33] showed that incidence of acne vulgaris in smokers was significantly lower than nonsmokers. Schafer et al. [34] and Chuh et al. [35] in their studies noted that smoking is likely to bear a positive correlation with acne. In our study, men who were smokers had more severe grade of acne vulgaris compared to nonsmokers. Since the number of smokers is small, no valid conclusion can be derived from this. Impaired vasoreactivity, relative ascorbic acid deficiency, impaired collagen synthesis and wound healing in smokers may play some part in the underlying pathogenesis for the association between smoking and acne. The improvement of acne in summer and exacerbation in winter is a conventional dermatological opinion. Studies done in the past have shown varied results regarding seasonal variation in acne vulgaris. A Saudi Arabian study has shown that acne exacerbates in winter, and often improves during the summer months. [5] An Indian study showed that majority of patients with acne vulgaris worsened during summer. [36] In our study, seasonal variation was observed only in 80 patients (25.9%); 71 patients (23%) exacerbated in summer and 9 (2.9%) in winter. This observation was against the conventional view that acne vulgaris exacerbates in winter and improves in summer. To conclude, our study included 309 patients with acne vulgaris, with the frequency of the disease being 1.068% of patients attending dermatology OPD. The mean age of the patients was 19.78 years and the male to female ratio was 1.25:1. In the older age group, women were more affected than men ( P = 0.001). Most patients were in the age group of 16-20 years (59.8%) and the majority being either college (33.3%) or school (33%) students. Face was involved in all cases and face involvement alone was observed in 202 (65.4%) cases. There were 186 patients (60.2%) with grade 1 acne vulgaris, 85 (27.5%) with grade 2 acne, 8 (2.6%) with grade 3 acne and 30 (9.7%) with grade 4 acne. Closed comedones were the predominant lesions, with the ratio of closed comedones to open comedones being 4.9:1 and the ratio of noninflammatory to inflammatory lesions as 8.55:1. Scarring and hyperpigmentation, the sequelae of acne, were observed in 39.5% and 24.6% of patients, respectively. Seventeen of our female patients (12.4%) had cutaneous markers of androgenicity and the most common marker was hirsutism (76.4%). The most common disease associated was seborrheic dermatitis (21.35%). Seasonal variation was observed only in 80 patients (25.9%); 71 patients (23%) exacerbated in summer and 9 patients (2.9%) in winter. Men who were smokers had a more severe grade of acne vulgaris compared to nonsmokers ( P = 0.001). This study brings out the clinical profile of acne vulgaris in a tertiary care hospital in South India. As this study is hospital based and carried out at a tertiary care center, future studies with more number of patients and even population-based studies can truly find the prevalence of acne vulgaris in our community. The drawback of this study was that female patients who had clinical markers of androgenicity were not explored for hormonal abnormality, if any. References
Copyright 2009 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv09081f4.jpg] [dv09081f1.jpg] [dv09081t4.jpg] [dv09081f5.jpg] [dv09081f3.jpg] [dv09081t1.jpg] [dv09081t3.jpg] [dv09081f2.jpg] [dv09081t2.jpg] |
| |||||||||


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}