 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
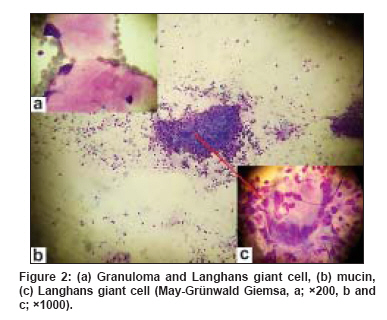
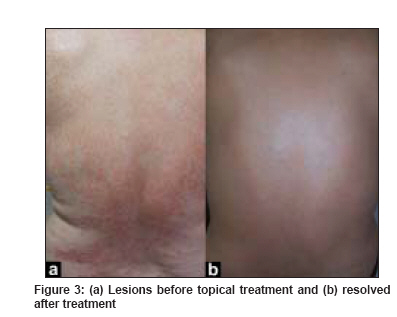
Indian Journal of Dermatology, Venereology and Leprology, Vol. 75, No. 3, May-June, 2009, pp. 287-289 Case Report Generalized granuloma annulare in a patient with myelocytic leukemia and chronic hepatitis B virus infection Ülkü Aşkõn,, Durdu Murat, Şenel Engin Department of Dermatology, Baskent University Faculty of Medicine, Ankara Code Number: dv09084 PMID: 19439883 Abstract Granuloma annulare is a granulomatous disorder of the dermis and subcutaneous tissue, with different clinical types. Generalized granuloma annulare is a rarely encountered clinical entity. We describe a 60-year-old woman with a 4-month history of generalized annular lesions. She had a history of myelocytic leukemia and chronic hepatitis B virus infection. To date, both acute myelocytic leukemia and hepatitis B virus infection have been described independently in association with generalized granuloma annulare but have never been described together in association with generalized granuloma annulare. Probable etiological causes of granuloma annulare are discussed in our patient.Keywords: Generalized granuloma annulare, Acute myelocytic leukemia, Hepatitis B, Tzanck smear Introduction Granuloma annulare (GA) is an idiopathic and benign granulomatous disorder with classic features including single or multiple papules with a tendency to form annular lesions. There is a wide spectrum of clinical subsets including localized, generalized, perforating, and subcutaneous types. Generalized granuloma annulare (GGA) is a rare variant of GA, observed predominantly in women aged 30 to 70 years. Although the pathogenesis of GGA is unknown, it has been described in patients with diabetes mellitus, malignancies, thyroid diseases, hepatitis B and C virus infections, medications, and acquired immunodeficiency syndrome. [1],[2],[3],[4] Here, we report GGA in a patient with a history of acute myelocytic leukemia and chronic hepatitis B virus (HBV) infection and describe the Tzanck smear findings of GA.Case Report A 60-year-old woman presented at our institution with a 4-month history of generalized annular lesions. The patient had been diagnosed as having acute myelocytic leukemia (AML M1-2) two years earlier and had been treated with chemotherapy (cytarabine); however, her leukemia did not respond to treatment. She also had chronic HBV infection for 2 years and had been treated with oral lamivudine (100mg/day) for 6 months. A dermatologic examination revealed symmetrical, generalized, yellow-brown-to-erythematous papules and annular plaques measuring 0.3 to 3cm distributed predominantly over her back, chest, and upper extremities [Figure - 1]. Histopathological examination showed that the mucin-positive granulomatous infiltrate included lymphocytes and multinucleated giant cells in the upper and mid-dermis. The results of biopsy staining and cultures for fungi and mycobacteria were negative. Polymerase chain reaction (PCR) analysis for HBV DNA was negative. A Tzanck smear disclosed granuloma with mucin and Langhans-type giant cell [Figure - 2]. The findings of histopathology and Tzanck smear were consistent with the diagnosis of GA. Results of serologic tests for hepatitis HBsAg and anti- HBe were positive, whereas those of HBeAg, anti- HBs and anti-HCV were negative. No significant changes were seen in renal, hepatic or thyroid function tests, or on a urine analysis. The serum glucose level was normal. Laboratory analysis demonstrated the following values: Hemoglobin, 10.9g/dL; leukocyte, 2680/mm 3 ; and platelet count, 4,91,000/mm 3 . Peripheral smear showed 5% atypical mononuclear cells. Bone marrow aspiration revealed blastic infiltration, dysmyelopoiesis and dyserythropoiesis. Results of a chest radiograph and abdominal ultrasonographic examination were normal. She was treated with a topical steroid (clobetasol propionate), and the skin lesions completely resolved 3 months later [Figure 3a] and [Figure 3b]. Treatment with cytarabine and lamivudine was continued. No recurrence was seen at 1-year follow-up. Discussion GA is a benign, usually self-limited, inflammatory dermatosis of unknown etiology. Clinical variants of GA are localized, generalized, subcutaneous and perforating. GGA is a rare variant that represents 8.5% to 15% of all cases of GA. GGA presents clinically with skin-colored, erythematous or violaceous dermal papules and/or small annular plaques with slightly elevated borders. In nearly 70% of cases, these plaques are asymptomatic, but they may cause pruritus or a burning sensation. The pathogenesis of GA is still not well understood. The antigenic stimulus that initiates the delayed-type hypersensitivity reaction is unknown, but various associations have been reported, which include diabetes mellitus, malignancies, thyroid diseases, hepatitis B and C virus infection, medications and acquired immunodeficiency syndrome. [1],[2],[3],[4],[5] Harman et al. , first reported an association of GA and malignancy in 1977. [6] Later, in a series of 100 patients with GGA, Dabski and Winkelmann found 14 cases of internal malignancies preceding or following the skin eruption; however, they rejected a causative relationship between the 2 disorders owing to the wide variation in time between their onsets. [2] The mechanism of the association between GA and malignancies is unknown. It is speculated that GA results from an immunologic reaction stimulated by an unidentified tumor antigen. These patients may have decreased cell-mediated immunity due to tumors. Tumor cells may directly or indirectly cause secretion of cytokines; cytokine activation of fibroblasts might produce an inflammatory reaction that mediates the formation of a granuloma. In addition to patients with malignancy and tumor-related immunodeficiency, GA has also been observed in individuals with deficiencies in cell-mediated immunity, such as patients with HIV infection [7] or sarcoidosis; [8] this suggests that immunologic factors may have a role in the development of malignancy-associated GA. In most patients with malignancy, a diagnosis of cancer had previously been established, and the appearance of GA lesions was not temporally associated with detecting an underlying malignancy. [1] Although uncommon, GA may be temporally associated with detecting a previously undiagnosed malignancy or recurrent metastatic disease, and resolution of the dermatosis may be temporally associated with successful treatment of that cancer. [1] Among the hematologic malignancies, malignant lymphoma has been commonly reported, but there is only one report in the literature of GGA with acute myelocytic leukemia. [9] In our patient, this association might have been coincidental, because the skin lesions resolved with topical treatment after 3 months, although the leukemia did not respond to treatment. There is one report in the literature of GGA associated with chronic HBV infection, suggesting a link between GGA and HBV infection, which was further confirmed by HBV-DNA in the biopsy papules of GGA. [4] Moreover, a GA-like eruption caused by chronic hepatitis C virus infection and hepatitis B vaccination has been reported.[10] In our patient, although the DNA of HBV in the biopsy specimen and the serum HBV DNA quantitative PCR assay showed negative results, the eruption also could have been caused by HBV infection that provoked a cellular immune response via T lymphocytes. The time interval between GA and cancer and HBV infection cannot be exactly evaluated, because both of these are usually asymptomatic during the early stages and are often ignored. Therefore, the association must be readily clarified by further studies and new case reports. The Tzanck smear can be used as a cytologic diagnostic tool for granulomatous diseases. The Tzanck smear will demonstrate granulomas and Langhans-type giant cells in sarcoidosis and tuberculosis. In our case, cytologic examination showed Langhans giant cells, granulomas and mucinous materials. The Tzanck smear findings were concordant with the histopathological findings and are the first such findings to be described in the literature for GA. In conclusion, GA with acute myelocytic leukemia and HBV infection is rare. Clinicians should be aware of underlying cancers, especially in elderly patients with GA. References
Copyright 2009 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv09084f2.jpg] [dv09084f3.jpg] [dv09084f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}