 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
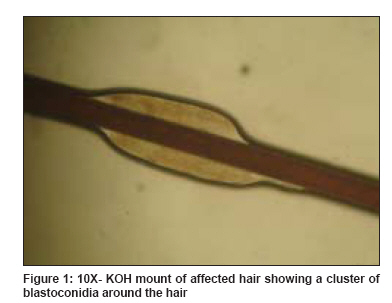
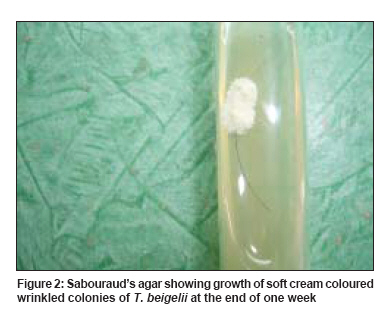
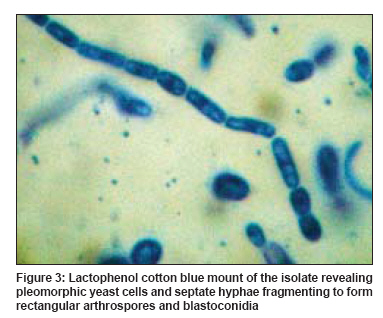
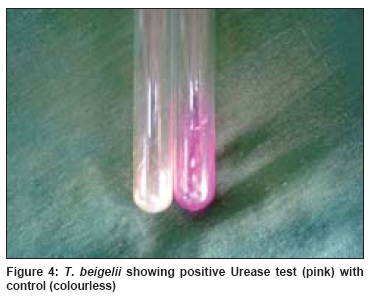
Indian Journal of Dermatology, Venereology and Leprology, Vol. 75, No. 3, May-June, 2009, pp. 293-295 Case Report Two cases of scalp white piedra caused by Trichosporon ovoides Tambe Swagata A., Dhurat S. Rachita, Kumar Chaya A., Thakare Preeti, Lade Nitin, Jerajani Hemangi, Mathur Meenakshi Department of Dermatology , Lokmanya Tilak Municipal Medical College and General Hospital, Sion Mumbai - 400 022 Code Number: dv09086 PMID: 19439885 Abstract White piedra is a superficial fungal infection of the hair shaft, caused by Trichosporon beigelii . We report two cases of white piedra presenting as brown palpable nodules along the hair shaft with a fragility of scalp hairs. T. beigelii was demonstrated in hair culture of both the patients and T. ovoides as a species was confirmed on carbohydrate assimilation test. The first patient responded to oral itraconazole and topical ketoconazole, with a decrease in the palpability of nodules and fragility of scalp hairs at the end of two months.Keywords: White piedra, Carbohydrate assimilation test, Itraconazole, Trichosporon ovoides Introduction White piedra is a superficial fungal infection of the hair shaft, caused by Trichosporon beigelii , also known as tinea nodosa, trichosporonosis nodosa and trichomycosis nodularis. [1] Common areas of involvement include distal portions of facial, beard, moustache and pubic hairs, with the scalp being rarely involved. [1] Infection appears to begin just beneath the hair shaft to form soft white to light brown easily detachable nodules, spaced irregularly along the hair shaft. They are microscopic, with about 0.5mm in diameter, producing a sensation of grittiness. Coalescence will result in a sleeve-like mass indistinguishable from trichomycosis axillaris. [2] The growth occurs as a collarette around the hair shaft and consists of mycelia that rapidly fragment into arthrospores. The hair is weakened at these points, and hence may break, resulting in split or frayed ends. [2] Case Report Two females, aged 32 and 23 years, presented for evaluation of palpable nodules along the scalp hairs with fragility for 3 and 2 months, respectively. Both the patients had a history of tying wet hairs after washing. Other hairy parts of the body were not similarly affected in both. Their family members had no similar involvement. Both had never visited southern parts of India or used oils excessively. Examination in both the cases revealed normal-looking scalp hair without evidence of sparseness. However, individual hair showed barely visible but well-palpable brownish nodules distributed at irregular intervals and not easily movable along the hair shaft. Hair pull test result was negative. Wood′s lamp examination of the affected hairs and hairs from other body parts did not show any fluorescence. Clusters of blastoconidia were present intermittently along the hair shaft on 10% KOH mount [Figure - 1]. Growth on Sabouraud′s agar at 37°C and 22°C revealed soft cream-colored wrinkled colonies at the end of one week [Figure - 2]. Lactophenol cotton blue mount of the isolate revealed pleomorphic yeast cells and septate hyphae fragmenting to form rectangular arthrospores and blastoconidia [Figure - 3]. Macroscopic findings, microscopic findings and urease test positivity [Figure - 4] confirmed the identity of isolate to be T. beigelii complex, the causative agent of white piedra. Carbohydrate assimilation test with inositol, l-arabinitol, sorbitol, raffinose, melibiose and xylitol confirmed the species to be T. ovoides . Case 1 was treated with topical ketoconazole shampoo for two weeks, with no improvement, requiring addition of oral itraconazole 100 mg once daily with a decrease in the palpability of nodules (concretions) and fragility of scalp hairs at the end of 2 months. The second case was lost to follow-up. Discussion White piedra belongs to family Cryptococcacaea, class Bassidiomycetes and is an uncommon infection of worldwide distribution seen in temperate and topical areas including Europe, Asia, Japan and southern United States. [1],[2] It was first described by Beigel in 1865 and the first case in India was reported by Basu et al. in 1970. [2] In India, most of the reported cases are from the southern region of India, [3],[4],[5] but isolated cases have been reported from Mumbai [5] and Delhi. [6] People of all age groups are affected, with a higher incidence in young women. [7] Age and sex incidence varies from country to country, depending on the prevalent hair dressing fashions and social customs. [2] Twelve patients in a study by Khandpur et al. and both the present patients are traditional burkha-clad Muslim women. [7] Whether the custom of covering hairs is a contributory factor needs to be studied. Mumbai being a humid, warm region, with constant perspiration, habit of tying wet hairs and custom of covering the hairs with veil prevent exposure to sunlight, which acts as a natural germicidal agent. All these taken together increase the chances and persistence of fungal infection, as fungi thrive in warm and humid environment. Length of scalp hair also correlates with an increased risk of acquiring white piedra, [8] as seen with our patients. T. beigelii is saprophytic yeast that dwells in air, soil, river, water, animal excreta and sewage. Mode of transmission in man is not clear. It colonizes the human skin and respiratory, urinary and gastrointestinal tracts and has even been isolated from hair of animals such as horses and monkeys. Colonization of human hair may occur as a consequence of poor personal hygiene, washing of hair in stagnant water, persistence of warm and moist conditions on the scalp, excessive use of hair oils and irregular combing habits. [7] An epidemiological study has shown that the disease predominantly affects scalp hair in tropical countries and pubic hair in temperate countries. [8] It is significant to note that our patients had involvement of only the scalp hair, with conspicuous sparing of the other areas. Gueho has subdivided T. beigelii into 6 species, which are pathogenic to humans. [2],[9] These are T. ovoides , T. inkin , T. mucoides , T. asteroides , T. ashii and T. cutaneum . Species identification is done by carbohydrate assimilation test. They have different ecologies. T. ovoides and T. inkin are the most frequently isolated species in white piedra. T. ovoides causes white piedra of the scalp, while T. inkin is largely detected in pubic piedra. T. asteroides and T. cutaneum are isolated less frequently in superficial lesions and in most cases are probably contaminants. [2] T. ashii causes hematogenously disseminated infections, while T. mucoides usually causes CNS involvement; seen in immunocompromised patients. Systemic infection can lead to fever, pneumonia, endocarditis, cellulitis, glomerulonephritis, endophthalmitis, brain abscess, otomycosis and onychomycosis. [2] Therefore, species identification becomes an important aspect wherever facilities are available. In present cases, T. ovoides was identified. There is paucity of literature on species identification in previous reports. The differential diagnosis is very important as, being very rare in Mumbai, white piedra can pass unnoticed or be mistaken for pediculosis. The differential diagnosis includes Pediculosis capitis , trichomycosis axillaris (recently renamed as trichobacteriosis), peripilar keratin cast, monilethrix and trichorrhexis nodosa. [2] Wood′s light examination, KOH mount and fungal culture help in differentiating these conditions. In trichomycosis axillaris, Wood′s lamp examination shows fluorescence, while other conditions show no fluorescence. KOH mount examination of hair shows hyphae and arthroconidia in white piedra, whereas coryneiform bacteria of trichomycosis axillaris cannot be visualized clearly. Fungal and bacterial cultures readily differentiate between the white piedra and trichomycosis axillaris. [1],[2] Shaving of affected hair is the most effective remedy but not acceptable in women. [1] Several topical and systemic antifungals have been tried with variable efficacy as noted by different authors. [1],[9] In our first patient, topical antifungal alone was ineffective, and addition of oral itraconazole produced dramatic improvement. Commonly used topical antifungals include ketoconazole, ciclopirox olamine shampoo, 2% selenium sulphide, 6% precipitated sulphur in petrolatum, zinc pyrithione and amphotericin B lotion. Oral agents used include ketoconazole and amphotericin B. [10] Recent reports show that itraconazole is also effective in the treatment of white piedra. [7] Oral azole antifungal agents eliminate the scalp carriage or infection, whereas antifungal shampoo eliminates the hair shaft concretions without the need for shaving. [9] References
Copyright 2009 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv09086f2.jpg] [dv09086f1.jpg] [dv09086f4.jpg] [dv09086f3.jpg] |
| |||||||||


{kind=link}
{kind=link}
{kind=link}
{kind=link}