 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
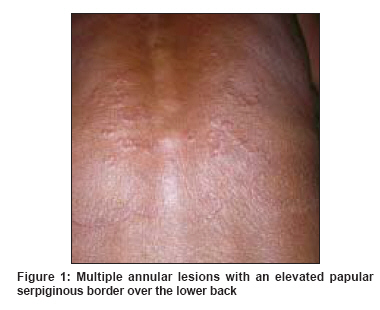
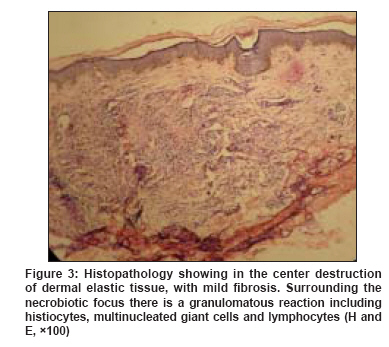
Indian Journal of Dermatology, Venereology and Leprology, Vol. 75, No. 3, May-June, 2009, pp. 296-299 Case Report Granuloma multiforme: A report from India Kumari Rashmi, Thappa DevinderMohan, Chougule Abhijit, Adityan Balaji Department of Dermatology and STD, Jawaharlal Institute of Postgraduate Medical Education and Research (JIPMER), Pondicherry - 605 006 Code Number: dv09087 PMID: 19439886 Abstract Granuloma multiforme (GM) is a reactive skin disorder of unknown etiology, characterized clinically by confluent annular lesions and histologically by focal necrobiosis and histiocytic granulomas. GM is significant because of its clinical resemblance to tuberculoid leprosy, with which it can be confused. Here, we report a case of granuloma multiforme from India in a 70-year-old male farmer, with multiple asymptomatic large annular rings of papules over the back and thighs on photodistributed sites. Histopathology helps to clinch the diagnosis and differentiate from similar clinical and histologic mimics such as granuloma annulare, tuberculoid leprosy, actinic granuloma and annular sarcoid. Nevertheless, a very high degree of suspicion is required to diagnose GM.Keywords: Granuloma multiforme, Annular lesions, Leprosy Introduction Leiker [1] in 1964 coined the term granuloma multiforme, "a disease resembling leprosy," to describe an entity with "a granulomatous structure and variation in clinical aspect." He described the profile of 148 such patients found in Nigeria in a survey. [1],[2],[3] Later similar cases were reported by Browne [4] from eastern Nigeria and Meyers et al., [5] from Congo. Most of these patients were found in leprosy settlement where they were mistakenly receiving treatment for leprosy. It has been reported mostly from African countries, [2],[3],[4],[5],[6] but rarely from other parts of the world. [7],[8] Granuloma multiforme (GM) is a reactive skin disorder of unknown etiology, characterized clinically by confluent annular lesions and histologically by focal necrobiosis and histiocytic granulomas. GM is significant because of its clinical resemblance to tuberculoid leprosy, with which it can be confused. Here, we report a case of granuloma multiforme from India, where although leprosy is very common the cases of GM are very rarely reported. Case Report A 70-year-old farmer from South India presented with asymptomatic multiple, ring-shaped lesions on his back and thighs of 2 weeks duration. There was no history of itching, scaling, burning or decreased sensation associated with the lesions. The largest lesion appeared first over the lower back followed by multiple, new, smaller ring-shaped lesions on the upper back and thighs. The lesions began as a papule and slowly developed central clearing with progressive increase in the size of some of the lesions over the last two weeks. There was no history of contact with leprosy patients. He worked in fields usually without a shirt because of excessive heat and wears only a loincloth. On examination, there were multiple annular lesions with an elevated serpiginous border. The largest plaques on the lower back measured 15 x 10 cm in diameter and the one on the right knee measured 6 cm in diameter [Figure - 1] and [Figure - 2]. Multiple, smaller annular lesions and red-colored papules were present asymmetrically distributed over the entire back. All lesions had a prominent erythematous to skin- colored, irregular, papular border, which was firm in consistency. There was central clearing without any hypopigmentation, atrophy or scaling. There was no loss of sensation over the lesions or peripheral nerve thickening. Systemic examination was normal. Clinical possibilities considered were granuloma annulare, granuloma multiforme and annular sarcoid. The result of slit skin smear was negative. Routine investigations, including hemogram, renal and liver functions, blood sugar levels, chest X-ray and urine examination were within normal limits. A skin biopsy was taken from the elevated edge of one of the larger lesions on the lower back to confirm the diagnosis. Histopathology showed a characteristic zonal histology. The center showed destruction of dermal elastic tissue, with mild fibrosis. In the raised active edge of the lesion, there was a granulomatous reaction, which includes histiocytes, multinucleated giant cells and lymphocytes. Elastic fibers were greatly reduced with elastoclasia; most of those that remained were fragmented. Areas of necrobiosis surrounded by palisaded rim of histiocytes in the mid and upper dermis were seen in the annular rim. No acid-fast bacilli (AFB) were detected. These findings were consistent with a diagnosis of granuloma multiforme [Figure - 3]. The patient was followed up for 12 weeks, without any resolution of the lesions after biopsy. He was advised to apply topical steroids but failed to show any improvement. Discussion Gosset [9] first noticed this entity in the early 1940s, but it was Leiker et al. [1] who first described GM and separated it from tuberculoid leprosy. It is called " Unono enyl" (elephant ringworm) in Africa. The condition was originally thought to be confined to Central Africa; however, it has been reported occasionally from Nigeria, [1],[2],[3],[4] Kenya, [3] Congo, [5] Tanzania, [7] Zaire, [7] Cameroon [7] and Indonesia. [7] The disease is found among adults over the age of 40 years, with a predilection for the female sex. The sun exposed sites of the upper trunk and arms are predominantly affected. The clinical picture varies considerably. The initial lesions are usually papules, which soon evolve to form annular and polycyclic lesions with papular or nodular edges. Elevated plaques may also be present. The lesions tend to last for months or years, extend with central healing, and often leave residual hypopigmented macules, but hyperpigmentation has also been noted in some reports. [5] It is pruritic and irritating, especially when new lesions are forming. Our case was an elderly man who had asymptomatic lesions, but evolution of lesions was very typical and all the lesions were over the photoexposed sites. Lesions of GM show no impairment of sweating, local sensation or nerve enlargement, which differentiate it from tuberculoid leprosy. The lesions also never ulcerate. The general health of the patient is not affected, but the disease is a cause of cosmetic disfigurement. Other conditions that should be differentiated from this rare granulomatous disorder include granuloma annulare, tuberculoid leprosy, sarcoidosis and necrobiosis lipoidica diabeticorum. GM is commonly seen after the age of 40 years. The clinical picture and skin biopsy findings help to establish the diagnosis and to differentiate it from other conditions. Larger lesions distributed on the neck and trunk in GM contrast with the smaller rings of granuloma annulare (GA) seen on the distal aspects of the limbs. GA is usually seen in children and women, with a predisposition for hands and feet. The lesions are usually asymptomatic. Histology shows foci of necrobiosis surrounded by granulomatous zone with elastotic material within the granulomas. The giant cells contain fewer nuclei and scarring is absent. Nerves are intact. Lesions respond to topical steroids or resolve spontaneously. GM differs from granuloma annulare in the dense perivascular infiltrate seen, the absence of mucin, the absence of palisading of cells and particularly the prominent larger and more number of multinucleate giant cells in the infiltrate. Complete loss of elastic tissue in the central zone, as seen in the GM is the primary basis for differentiating GM from plaque GA. Tuberculoid leprosy lesions may be hypopigmented, ichthyotic with hypoanesthesia and peripheral nerve thickening. Histopathology shows granulomas in all the layers of dermis and there is no collagen degeneration. Perineural and perivascular infiltrates are seen, with occasional acid fast bacilli within the nerve on Fite Faraco staining. Lesions respond to antileprosy treatment. [1] Annular elastolytic giant cell granuloma or actinic granuloma is very similar in clinical presentation, occurring in older individuals over the sun-exposed areas as annular plaques. It can be differentiated on the basis of histology. Although, a similar zonal pattern is seen with a granulomatous response with multinucleated giant cells at the rim the (nuclei, 12) and centrally a loss of elastotic material and scarring, but unlike GM, necrobiosis is not usually seen and there is no mucin deposition in the dermis. But recently, many authors have called GM lesions to be same as actinic granuloma. Atypical necrobiosis lipoidica shares many histological features with GM, the distinguishing features are the presence of fibrosis intermingled with the necrosis, vessel wall changes and fat deposition. Clinically, these are annular lesions over the upper face and scalp seen in women around the age of 35 years and unlike necrobiosis lipoidica, they heal without scarring or alopecia. Annular granulomatous lesions in ochronosis due to hydroquinone have been reported from South Africa. The lesions occur over face resemble actinic granuloma histologically. Clinically, there is a central area of hypopigmentation, followed by an elevated rim and an outside ring of ochronotic hyperpigmentation. Annular sarcoid is another entity to be differentiated from GM histologically but usually naked granulomas are seen, which easily differentiate it from GM. The etiopathogenesis of GM is still unknown. No bacteria or any other infectious agent has been identified. [1],[2],[4],[5] Airborne agents, dust, organic excreta and irritant material have been considered as the cause of granulomas but not proved. Recently, it has been proposed that GM is a photodermatosis, and it has been postulated that the primary event in the pathogenesis could be cumulative damage to collagen. [10] This damage to collagen could be induced by a chemical or biological agent in the environment and further potentiated by immunologic factors. This is supported by the fact that, in almost all cases reported in the literature, including our patient, the lesions have been confined to sun-exposed areas. Regan [11] has also supported this observation and referred to these lesions as being similar to actinic granuloma and would suggest that actinic radiation plays a significant role in the etiology of these lesions due to elastosis/elastolysis of photo-damaged elastin. Unfortunately, no effective therapy is available for this disorder. Clarification of the cause and pathogenesis of granuloma multiforme awaits further clinical and pathologic studies. A trial of topical steroids failed to have any benefit in our case. Although, leprosy is so endemic in India reports of GM from this tropical country are very few. This is only the third report of this disorder from India; the first two cases were reported by Cherian [8] from South India and the third from North India. [12] Probably, many cases are still being misdiagnosed as leprosy and hence underreported. This report emphasizes that this rare entity is not confined to Africa, as initially thought, and should be kept in mind in the differential diagnosis of annular granulomatous disorders. References
Copyright 2009 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv09087f1.jpg] [dv09087f3.jpg] [dv09087f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}