 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
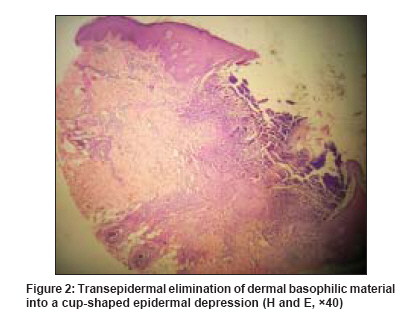
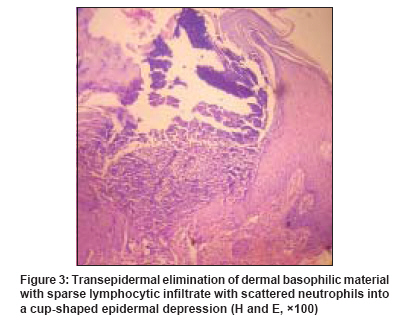
Indian Journal of Dermatology, Venereology and Leprology, Vol. 75, No. 3, May-June, 2009, pp. 306-307 Letter to the Editor Acquired reactive perforating collagenosis following insect bite Ghosh SudipKumar, Bandyopadhyay Debabrata, Chatterjee Gobinda Departments of Dermatology, Venereology, and Leprosy, R.G. Kar Medical College, Kolkata Code Number: dv09092 PMID: 19439891 Sir, Reactive perforating collagenosis (RPC) is a rare skin disorder characterized by transepidermal elimination of altered collagen through the epidermis. Two distinct patterns of the disease exist; the inherited form manifesting during childhood and the acquired form occurring in the adults. [1] We report here a case of acquired RPC after insect bite for its rarity and to emphasize the importance of considering RPC in the differential diagnoses of umbilicated papules or other perforating disorders. A 22-year-old woman presented with a few gradually developing, itchy, reddish small swellings on her arms, forearms, and hands for the last 4 months. There was no history of vesiculation, oozing, or crusting. Some of the elevated lesions healed spontaneously with scarring. She recalled having developed several extremely pruritic reddish tiny lesions after some insect bites on the same locations during an excursion to a forest area about a month before the onset of the present illness. The insect bite reaction subsided spontaneously within a few days without any specific treatment. Examination showed multiple, slightly erythematous, dome-shaped umbilicated papules with a diameter of 2 to 4 mm with central adherent keratotic plugs [Figure - 1] on her arms, forearms, and the dorsal aspects of the hands. A few shallow atrophic scars were also visible around the lesions. The skin in general was otherwise normal in appearance. Examination of the nails and mucosae showed no abnormality. Systemic examination was unremarkable. Investigations including complete hemogram, blood sugar, urea, creatinine level, liver function tests, and ultrasonography of the abdomen were normal. Excisional biopsy of a papule showed the evidence of transepidermal elimination of basophilic fragmented dermal material through a cup-shaped epidermal depression [Figure - 2]. A sparse lymphocytic infiltrate with scattered neutrophils was also noticed in the papillary dermis [Figure - 3]. On the basis of clinical and histological findings, a diagnosis of acquired reactive perforating collagenosis (RPC) was made. RPC is clinically characterized by umbilicated papules with a central adherent keratotic plug. Pruritus is common and the Koebner phenomenon may occur. Histology of the lesions is characterized by transepidermal elimination of altered dermal collagen bundles into a cup-shaped epidermal depression. [2] The term acquired perforating dermatosis instead of acquired RPC has also been suggested by some authors.[3] RPC after insect bite has very rarely been reported in the literature. [4] The lesions of RPC may appear after trauma, folliculitis or cold exposure as well as in association with multiple disorders, which include diabetes mellitus, renal failure, hyperparathyroidism, liver disease, neurodermatitis, IgA nephropathy, periampullary carcinoma with jaundice, adenocarcinoma, and liver neoplasms. [3] No systemic association could, however, be documented in our patient. Comprehensive diagnostic criteria of the disease exists. [1] Our patient fulfilled all the criteria for acquired RPC, in the form of histopathologic findings of elimination of necrotic basophilic material into a cup-shaped epidermal depression, clinical presentation of umbilicated papules or nodules with a central adherent keratotic plug and onset of skin lesions after the age of 18 years. All forms of RPC have the common feature of pruritus of varying severity, and it is likely that the transepidermal elimination of collagen is simply a reaction pattern as a result of chronic scratching or rubbing in a subset of pruritic patients. [3] The condition is often resistant to treatment. Control of pruritus is the cornerstone of management. Topical glucocorticoids, retinoids, keratolytics, systemic antihistamines, photochemotherapy, UVB phototherapy, liquid nitrogen cryotherapy, electrical nerve stimulation, and allopurinol, have all been tried with varying degrees of success. [3] Our patient was treated with oral antihistamines and topical tretinoin (0.05%) twice daily. Within six weeks, the lesions started to resolve but the patient was subsequently lost to follow-up. References
Copyright 2009 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv09092f1.jpg] [dv09092f2.jpg] [dv09092f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}